

Treatment options
Before administering any therapy, patients should be educated on proper foot hygiene to ensure a cool and dry environment in the shoe, and to trim and file nails to ensure good drug delivery.
Topical antifungal therapy
A variety of topical antifungal treatments are available. Ciclopirox and amorolfine are the two active ingredients considered to be most effective against a wide spectrum of dermatophytes, yeasts, and saprophytic molds. Ciclopirox is a mitochondrial enzyme chelating hydroxypyridone derivative15, while amorolfine is a fungicidal morpholine derivative 16.
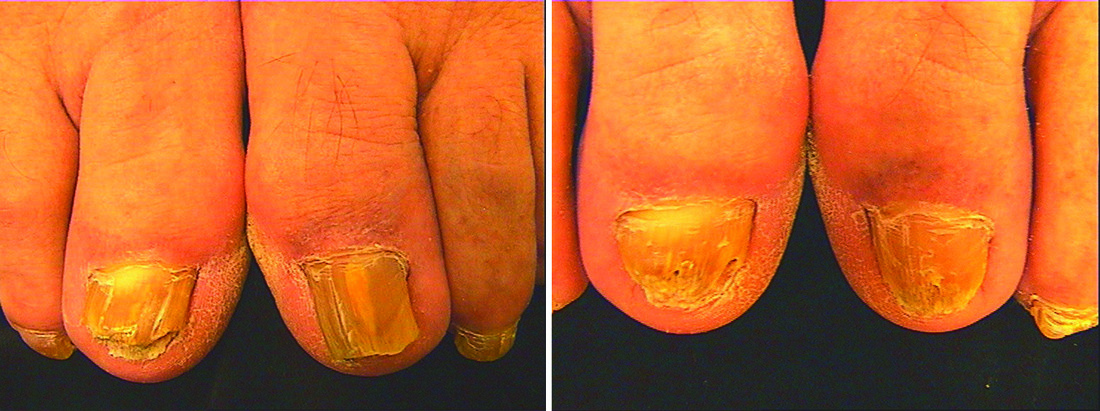
Figure 1 (left) Patient prior to treatment and (right) after five sessions 3 weeks apart with two passes of a 1450 nm 10 J laser
The primary difficulty in topical therapy is drug delivery into and below the nail. Only transungual drug delivery systems in a lacquer medium are able to deposit a significant amount of active ingredients in the affected nail and therefore be present for a longer time in therapeutic concentrations. However, the efficacy of nail lacquers is low: 38% cure rates for amorolfine and 25% for ciclopirox lacquers. Involvement of more than two thirds of a nail plate or lunula is associated with a poor response rate, and drug penetration through the nail plate is still an area for enhancement. Iorrizzo et al summarised indications for topical treatment of onychomycosis as17:
-
Distal subungual onychomycosis with less than 50% of nail involvement
-
Superficial white onychomycosis
-
Mold aetiology
-
Patients unable to tolerate oral therapy.
The main advantages of topical treatments are safety for patients and the absence of any severe
adverse drug reactions. This therapy option is appropriate for long-term prophylaxis of recurring onychomycosis18.
Systemic antifungal therapy
Systemic antifungal therapy is currently considered the most effective in treating onychomycosis. There are a number of antifungal drugs, which can be administered orally or intravenously: terbinafine, itraconazole, fluconazole, griseofulvin, ketoconazole, posaconazole, and ravuconazole. Among them, terbinafine is considered the most effective.
Terbinafine is a fungicidal allylamine derivative19, which inhibits ergosterol biosynthesis. A meta-analysis of 36 studies comparing available systemic monotherapies for onychomycosis reported the following mycological cure rates20:
-
Terbinafine = 76%
-
Griseofulvin = 60%
-
Itraconazole = 59%
-
Fluconazole = 48%.
Terbinafine (250 mg daily for 6–12 weeks) can be effective against dermatophytes in onychomycosis, but for Candida albicans it is only fungistatic21, and has a lower effectiveness against Scapulariopsis genera 22. Itraconazole should be the first choice for non-dermatophyte infections, and should be used in pulse therapy, to avoid adverse drug effects 23.
Terbinafine is reported to have the lowest number of adverse effects (metallic taste, diarrhoea, dyspepsia, nausea24) compared with other systemic medications. Since terbinafine, like many other drugs, is metabolised by the cytochrome P450, significant drug interactions may occur and the liver tissue might be stressed 24. It is recommended to discontinue the drug if elevation of alanine transaminase or aspartate aminotransferase serum levels persist.
However, systemic antifungals are still the first line therapy in most cases of onychomycosis. This is particularly true after 6 months of ineffective topical treatment, although patients with liver disease or possible drug interactions need other therapeutic options. Nail avulsion is usually no longer performed.

