


Fernando Felice outlines his treatment approach to restore volume to the periorbital region with the aid of hyaluronic acid fillers
When we attempt to rejuvenate a facial area, we must bear in mind not only the ageing process for the area to be treated, but also the ageing process for all areas involved — which anatomical structures are compromised and to what extent?
The periorbital region possesses a complex anatomy; therefore, the ageing of the area is multifactorial.
 We must adopt a multilayer approach when considering treatment options. This means we must give the correct treatment to the skin, the subcutaneous cellular tissue, and the muscular and bone layers.
We must adopt a multilayer approach when considering treatment options. This means we must give the correct treatment to the skin, the subcutaneous cellular tissue, and the muscular and bone layers.
Many patients, exclusive of their age, suffer noticeable ageing in their periorbital region, especially in the lower area. For the practitioner, approaching this area is not just about placing fillers wherever a depression is observed. The ageing process is multifaceted and this is how we must think when treating each one of our patients.
The cheeks support the periorbital area; consequently, symptoms of ageing will affect the whole cheek area rather than smaller portions. If, through ageing, the cheeks undergo subcutaneous cellular tissue atrophy as well as cutaneous muscular flaccidity, the result will be a loss of volume and downward movement due to the effects of gravity. This will result in a lack of support of the periorbital region and an increase to the height of the lower eyelid.
As a rule, when we decide to perform a treatment in the periorbital region, it is necessary to work on the malar and cheek areas.
Case analysis
Here we analyze the case of a 43-year-old man who presented with an inferior periorbital region. In our practice, we always perform a facial evaluation from five different angles: entire left profile, three-quarters left profile, frontal view, entire right profile, and three-quarters right profile.
The epidermal skin shows no signs of significant ageing and there is no noticeable skin excess. Muscle dynamics appear normal and there is no marked bone resorption.
From our analysis we can determine a treatment must be performed to fill the cheek and malar regions, as well as a second phase filling for the lower periorbital area. This will initially provide support and then treat the periorbital area. Both treatments can be performed on the same day, although we must always begin with the cheek and malar areas, and only after can we address the periorbital area.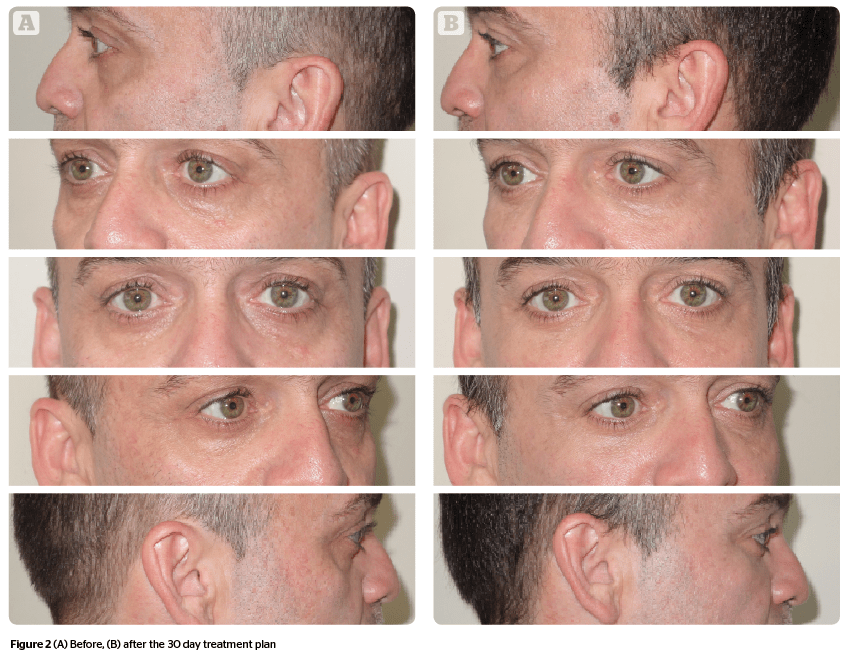
Treatment plan
The first stage of the treatment consists of improving the lower periorbital area support. It is vital to perfectly know the facial anatomy.
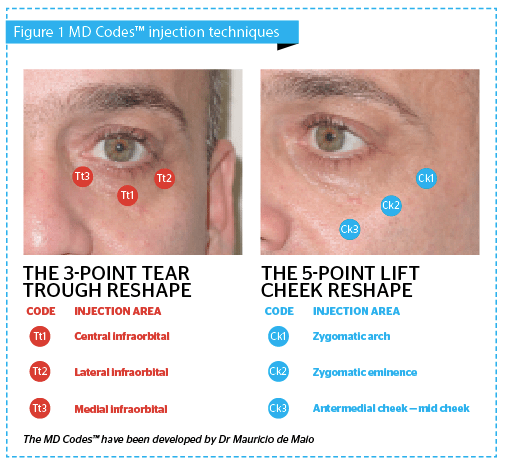
Following the rejuvenating codes described by Dr. Mauricio De Maio (MD codes™), we must start our treatment plan by the Ck1 (zygomatic arch), Ck2 (zygomatic eminence), and Ck3 (anteromedial cheek — mid-cheek) points followed by the Tt1 (central infraorbital), Tt2 (lateral infraorbital), and Tt3 (medial infraorbital) points (illustrated in Figure 2).
With this patient we used 0.5 ml of Juvederm Voluma® on each side to treat Ck points:
- Ck1 right=0.1 ml
- Ck2 right=0.1 ml
- Ck3 right=0.3 ml
- Ck1 left=0.1 ml
- Ck2 left=0.1 ml
- Ck3 left=0.3 ml
Points Ck1 and Ck2 must be applied in contact with the bone, exerting a slight traction upwards and backwards from the skin before applying. With this method, we achieve a lifting effect in the area. However, before injecting these points, we must aspirate due to the proximity of the zygomaticofacial artery and veins.
Ck3 must be applied in the subcutaneous layer as the goal is to replace the subcutaneous cellular tissue that was lost with ageing. Each application was performed pinching the skin perpendicularly, always after aspirating. This, again, is very important due to the proximity of the infraorbital artery and veins to Ck3.
Once the periorbital area support has been improved, we continue working with the Tt points in the lower orbital area.
- Tt1 right=0.2 ml
- Tt2 right=0.2 ml
- Tt3 right=0.1 ml
- Tt1 left=0.2 ml
- Tt2 left=0.2 ml
- Tt3 left=0.1 ml
This portion of the treatment was implemented while pinching perpendicular to the skin until touching the bone layer with the top of the needle. In that same location, after aspirating with the syringe, the product was placed in the retromuscular layer. Special care must be that the application is performed 1–2 mm below the lower orbitary edge because above the orbital rim is the orbital septum and behind it the infraorbital fat. If we place the product into the infraorbital fat, we would worsen the periorbital lower depression and the solution to this problem would be more difficult. The product used for the lower orbital area was Juvederm Volbella®.
 Once the treatment is completed it is important to tell the patients they may experience swelling in the treated area for at least one week.
Once the treatment is completed it is important to tell the patients they may experience swelling in the treated area for at least one week.
I recommend all patients that have undergone more than 2 ml of product to take one pill of ibuprofen 400 mg for pain management.
Conclusion
If we think in terms of multilayer ageing when we approach patients, it will allow us to offer a complete treatment and not only address specific facial areas.
Knowledge of the fat compartments of the malar and cheek area as well as the anatomy of the inferior orbital area is essential in order to obtain good results. I have found the technique described by Dr. Mauricio De Maio (MD Codes) to be very safe and practical, although other techniques do exist.
Always take into account areas where complications are more likely; a good technique is to always aspirate before injecting a filler to avoid an intravascular embolism (arterial or venous).




