

Brian S. Biesman and Molly E. Katz discuss their comprehensive approach to treating acne scars, including boxcar, atrophic, and pitted subtypes
 Acne scarring is a source of great distress and anxiety for affected patients. Regardless of age, gender or ethnicity, afflicted individuals are typically distressed by the appearance of their skin to the point that their self-confidence is affected, sometimes profoundly1-3. These patients are typically willing to undergo almost any recommended treatment in an effort to improve the appearance of their scars but are, unfortunately, frequently disappointed in their treatment outcomes. There are many reasons patient expectations remain unmet following acne scar treatment, including failure to identify the type of scarring correctly, failure to match the treatment with the scar type(s) present, improper performance of treatments, and failure to communicate realistic treatment outcomes. The treatment of acne scarring is currently in a state of evolution due to the recent introduction of new products and technologies, which now allow practitioners to offer more therapeutic options and better outcomes than what has previously been possible.
Acne scarring is a source of great distress and anxiety for affected patients. Regardless of age, gender or ethnicity, afflicted individuals are typically distressed by the appearance of their skin to the point that their self-confidence is affected, sometimes profoundly1-3. These patients are typically willing to undergo almost any recommended treatment in an effort to improve the appearance of their scars but are, unfortunately, frequently disappointed in their treatment outcomes. There are many reasons patient expectations remain unmet following acne scar treatment, including failure to identify the type of scarring correctly, failure to match the treatment with the scar type(s) present, improper performance of treatments, and failure to communicate realistic treatment outcomes. The treatment of acne scarring is currently in a state of evolution due to the recent introduction of new products and technologies, which now allow practitioners to offer more therapeutic options and better outcomes than what has previously been possible.
The keys to successfully treating acne scars lie in the accurate identification of patient concerns; proper characterization of the types of scars present, as each scar type responds best to a unique therapeutic approach; and determination of outcome expectations. A customized treatment plan can be made only when all of these factors have been considered. Other factors that may affect development of a treatment plan include Fitzpatrick skin type, presence of skin laxity, the relative risk/benefit ratio of each treatment, the amount of downtime associated with each recommended procedure, and the associated costs.
Assessment of scar type
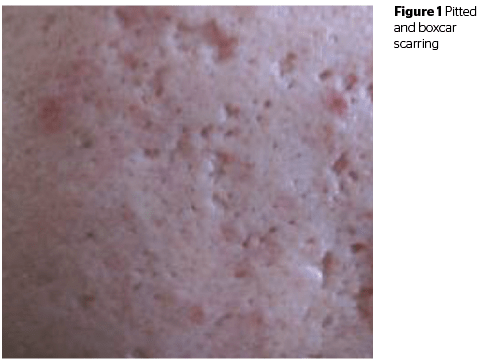
Assessment of scar type is critical when formulating a treatment plan as no modality or procedure is effective in improving the appearance of all scar types. Acne scars are typically categorized into rolling, boxcar, and ice-pick subtypes4 (Figure 1); we also believe that atrophic scarring is particularly common. It is helpful for physicians to have a general treatment approach for each scar type. There are often a number of potential options that could reasonably be employed when treating acne scars; the goal of this article is not to offer a comprehensive review but to simply share our approach.
The consultation process
P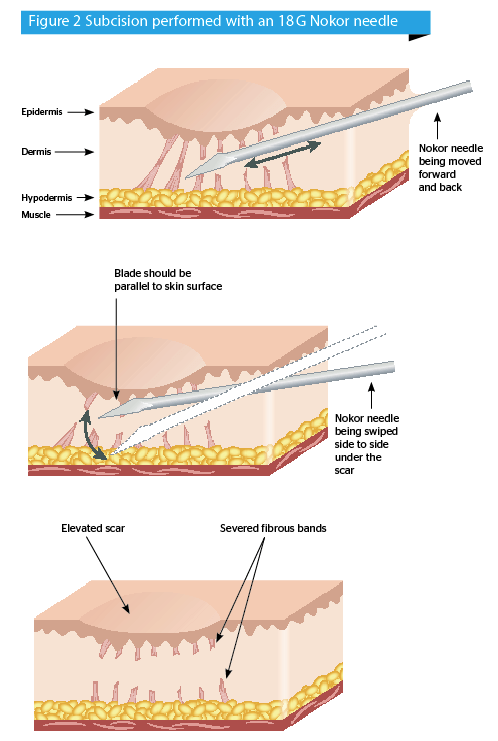 rior to making a treatment recommendation, it is critical to spend adequate time during the consultation to understand what is required. Many acne scar patients have undergone one or more treatments that have left them disappointed or unhappy. In our experience, most of these cases involve patients who have been treated with technologies or procedures that could not have reasonably been expected to produce significant clinical improvement. Understandably, these patients are frequently hesitant to proceed with additional treatments out of fear of again not achieving their desired outcome. The psychological impact of acne and acne scarring cannot be overstated. Patients who suffer from acne scarring tend to be highly conscious of their scars and have low self-esteem as a result. Subsequently, these patients are typically desperate for improvement and therefore willing to undergo nearly any procedure that is recommended. Great care must be taken not only to formulate a treatment recommendation that is likely to produce a significant improvement but also to communicate reasonable expectations about the outcome.
rior to making a treatment recommendation, it is critical to spend adequate time during the consultation to understand what is required. Many acne scar patients have undergone one or more treatments that have left them disappointed or unhappy. In our experience, most of these cases involve patients who have been treated with technologies or procedures that could not have reasonably been expected to produce significant clinical improvement. Understandably, these patients are frequently hesitant to proceed with additional treatments out of fear of again not achieving their desired outcome. The psychological impact of acne and acne scarring cannot be overstated. Patients who suffer from acne scarring tend to be highly conscious of their scars and have low self-esteem as a result. Subsequently, these patients are typically desperate for improvement and therefore willing to undergo nearly any procedure that is recommended. Great care must be taken not only to formulate a treatment recommendation that is likely to produce a significant improvement but also to communicate reasonable expectations about the outcome.
The role of patient education during the consultation process cannot be overstated. We typically inform our acne scarred patients that there is no single treatment that is likely to produce an optimal outcome. We advise our patients that treatment should be viewed as a marathon not a sprint. We also advise patients that the goal of treatment should be an improvement in the global skin appearance and that, even after multiple procedures, there will still be some evidence of scarring. While most patients are thrilled at the prospect of any noticeable degree of improvement, those patients with unrealistically high expectations should not be treated. As is generally the rule in any aesthetic treatment, under-promising and over-delivering is the mantra by which these patients must be treated. On a positive note, producing improvement in the appearance of acne scars often leads to a dramatic improvement in self-esteem, which is reflected in many areas of a patient’s life.
Our approach to the treatment of acne scars by scar subtype
Diffuse erythema
Some patients who present acne scar treatment are more concerned about erythema (skin redness and inflammation), rather than scar texture or depression. It is important to ensure that the patients are not using topical products that are likely to contribute to inflammation. If the topical treatment regimen is appropriate and optimized, we typically treat erythematous scars with a long pulsed dye laser. In patients who have dyschromia related to photoaging as well as erythematous acne scars, intense pulsed light may be used.
Pitted scars
 Deeply pitted scars can be challenging to treat with any modality. In our experience, punch excision with closure is more successful than other approaches in producing improvement in deeply pitted scars. Patients are advised that subsequent laser skin resurfacing may well be required to help the linear scar heal more smoothly. Areas such as the nose, forehead, and medial midface sometimes do not respond as favourably to punch excision as the lateral cheeks due to the thicker, more sebaceous nature of the skin in these areas. Fortunately, pitted scars are less common than other subtypes.
Deeply pitted scars can be challenging to treat with any modality. In our experience, punch excision with closure is more successful than other approaches in producing improvement in deeply pitted scars. Patients are advised that subsequent laser skin resurfacing may well be required to help the linear scar heal more smoothly. Areas such as the nose, forehead, and medial midface sometimes do not respond as favourably to punch excision as the lateral cheeks due to the thicker, more sebaceous nature of the skin in these areas. Fortunately, pitted scars are less common than other subtypes.
Rolling scars
Rolling scars are the most common form of scarring seen in our patients. Clinically significant rolling scars vary in severity from mild to severe. Very mild rolling scars can 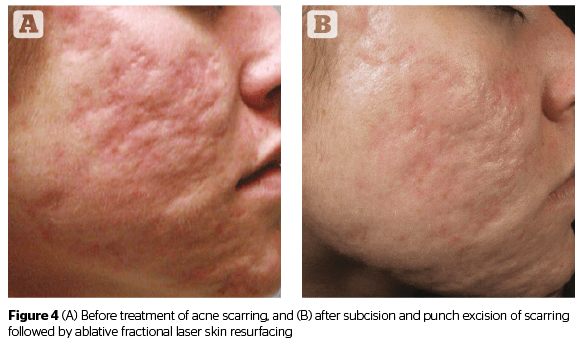 frequently be treated with a series of non-ablative fractional laser procedures. We typically treat more advanced rolling scars with aggressive subcision performed with an 18G Nokor needle5. Subcision is performed under local anesthesia (Figure 2). Patients typically report subjective improvement in the appearance of rolling scars from between 30–90% with an average of approximately 75%. In some scenarios, subcision can be performed more than once. Should additional improvement be desired following subcision of moderate to severe rolling scars, then fully ablative or ablative fractional resurfacing may be performed in patients with Fitzpatrick skin type I–III. For patients with darker skin types, bipolar radiofrequency resurfacing or aggressive microneedling can be performed. Once maximum improvement has been achieved using surgical and technology-based options, should there be residual areas of depression, injectable treatment using either hyaluronic acid for temporary improvement or collagen coated PMMA microspheres for long-term improvement is typically employed to achieve the best outcomes.
frequently be treated with a series of non-ablative fractional laser procedures. We typically treat more advanced rolling scars with aggressive subcision performed with an 18G Nokor needle5. Subcision is performed under local anesthesia (Figure 2). Patients typically report subjective improvement in the appearance of rolling scars from between 30–90% with an average of approximately 75%. In some scenarios, subcision can be performed more than once. Should additional improvement be desired following subcision of moderate to severe rolling scars, then fully ablative or ablative fractional resurfacing may be performed in patients with Fitzpatrick skin type I–III. For patients with darker skin types, bipolar radiofrequency resurfacing or aggressive microneedling can be performed. Once maximum improvement has been achieved using surgical and technology-based options, should there be residual areas of depression, injectable treatment using either hyaluronic acid for temporary improvement or collagen coated PMMA microspheres for long-term improvement is typically employed to achieve the best outcomes.
Boxcar scars
Boxcar scars are typically more atrophic and depressed than rolling scars. In our experience, boxcar scarring sometimes responds to aggressive subcision. If punch excision is being performed simultaneously for the treatment of ice pick scars, dermal grafts can sometimes be placed in the subcision pocket created under deeper boxcar scars. Boxcar scars can require surgical excision depending on their size, location, and the relative atrophy of the overlying skin. Shallower boxcar scarring with relatively good skin quality can respond well to nonsurgical treatment whereas deeper, larger, or more atrophic scarring may require surgical treatment for best outcomes. Injectables can be used to correct the appearance of boxcar scars especially in the absence of significant cutaneous atrophy.
Atrophic scarring
Atrophic acne scarring is often best treated with ablative fractional laser skin resurfacing. Multiple treatment sessions are often required. Ablative fractional resurfacing can also be performed depending on the relative severity of the atrophic scarring and the nature of other scars present. Many patients with atrophic scarring also benefit from the addition of poly-L-lactic acid (PLLA) either administered as an injection or applied topically at the time of ablative fractional resurfacing.
As most patients have a variety of different scar subtypes present, combination treatment is usually required to achieve best outcomes (Figure 3).
Other factors to consider when treating acne scarring
Presence of active lesions
Ideally, acne scar treatments shouldn’t be performed in the absence of active inflammatory lesion or cysts. Cystic lesions should not be present in the area where surgical subcision or excision is to be performed. If inflammatory lesions are present despite medical therapy, vascular laser therapy may be considered. Ablative fractional resurfacing and aggressive microneedling should not be performed around active inflammatory lesions.
Acne scarring in the presence of ageing skin
Acne scars can sometimes become more apparent with increasing skin laxity related to ageing and photoaging. This is one of the few clinical scenarios in the treatment of acne scarring in which we will offer ablative skin resurfacing as a first line treatment, as this will produce substantial improvement in skin laxity, reversal of photoaging changes, and improvement in the appearance of scarring.
The role of injectable fillers in the improvement of acne scarring may be relatively more important in patients who have volume depletion and loss of dermal collagen and elastin. As volume loss occurs, the acne scars have less support from the underlying soft tissue and can become more evident. In these cases, revolumization using soft tissue fillers is an essential component to achieving a successful outcome. PLLA is often used subcutaneously to both improve laxity as well as reduce the appearance of scarring. Soft tissue fillers may be used in conjunction with laser skin resurfacing in these patients. Superficially placed temporary injectable fillers including collagen and hyaluronic acid have been used extensively for the improvement of acne scars. In 2015, a long lasting injectable comprised of collagen coated PMMA (Belafill, Suneva, Inc.) was FDA approved for the treatment of acne scarring.
Microneedling
Microneedling of acne scars has been anecdotally reported to result in the improved clinical appearance of a variety of different acne scar types. As of yet, there is limited clinical data to support the use of microneedling for the treatment of acne scarring and it is important to note that microneedling does not have any FDA indication6. Anecdotally, in our experience, aggressive microneedling performed with either a manual or a powered device can result in significant clinical improvement in the appearance of all subtypes of acne scars including extensive pitted scarring that has been resistant to other treatment modalities. The depth of treatment is adjusted to correlate with the thickness of scarring and the anatomic region of the face being treated. Several treatments will be required to achieve the best outcome. Even with extensive treatment at depths of 2–3 mm, recovery with return to normal activities typically requires 3–5 days. It appears that microneedling can be used safely in patients with darker Fitzpatrick skin types. We currently do not use microneedling as a first-line treatment for acne scarring but continued to explore this versatile and relatively novel treatment to determine its ultimate role.
Acne scarring can have devastating psychological effects on affected individuals. Due to the fact that a variety of scar types are typically present in any given patient, a combination of approaches are typically required to achieve best outcomes. The practitioner treating acne scarring should have a complete understanding of the various modalities available to treat acne scarring, should understand the indications and the risks and benefits of each, and be able to set expectations appropriately. The treatment and improvement of acne scars can truly transform a person’s life.


