Daniel Sister explores the physiology of the aging face and explains how non-surgical treatments can deliver the desired results without the downtime associated with more invasive procedures.
A non-surgical facelift is now a realistic option for patients who desire to fight the aging process without resorting to surgery. In this article, the author looks at how and why the face ages, and addresses how a younger looking face can be achieved using non-surgical techniques.
The aging process of the face is complex and develops with a domino-like effect. It’s a three dimensional process that affects not only the skin, but also constantly interacts with the underlying layers: adipose tissue, muscles, and bones. This process is often described as the ‘cascade effect’. Aging can be attributed to:
- Laxity and ptosis of subcutaneous tissues
- Gravity
- A decrease in collagen and hyaluronic acid
- Atrophy and hypertrophy of adipose tissues
- Bone reabsorption
A lack of elasticity (due to loss of elastin), alterations in the texture of the skin, and muscular relaxation1,2.
The bone and cartilaginous structures become more visible as the skin and subcutaneous tissues get thinner, the texture of the skin is altered and convexities turn into concavities (temporal, perioral, and orbital areas).
- Further evident signs of aging include:
- Rhytids, lines, and folds
- Volume loss resulting in sagging skin
- Skin pigment changes
- Modifications in the face proportion.
In order to achieve a harmonious rejuvenation it might be necessary to adopt a multi-dimensional approach based on all or some of the following:
- Botulinum toxin
- Hyaluronic acid and/or other type of dermal fillers
- Platelet rich plasma (PRP or plasma therapy)
- ‘Bi-directional’ suspension sutures
- Bipolar radiofrequency (RF) energy
- Chemical peels.
This is how we can achieve ‘invisible lifting and rejuvenation’ without resorting to surgery.
The aging process
Understanding the aging process and how each different component (skin, muscle, fat, bones) is modified and/or altered by the aging process allows practitioners to specifically design the best combined treatments to achieve optimum results.
The face can be divided into three horizontal sections (upper third, middle, and lower third). In a young person there is a near perfect proportion between these three parts. However, the aging process will cause:
- Elongation of the upper third (consequence of hypotrophy of bone-cartilaginous tissue and ptosis of the soft tissues)
- The middle third appears to shrink due to the same causes
- In the lower third, there is a reduction in height because of the loss in the mandibular and maxillary bone structures, thinning of the skin and subcutaneous tissues as well as an increase in width because of ptosis of the middle third.
- The face can also be divided into three vertical sectors3
- Pro-face: central part of the forehead, nose, medial part of the lip and chin. Soft tissues are firmly anchored to the bone structures by means of strong and short ligaments
- Meso-face or intermediate sector: made of muscles and adipose tissues. The soft tissues not supported by efficient ligamentous structures are more prone to ptosis
- Meta-face: tissues are firmly anchored to the deep planes.
Skin
As we age the superficial and subcutaneous layers of the skin become thinner, this is a result of:
- Chrono-aging resulting in a reduced presence of collagen in the dermis
- The loss of elastin fibre structure, which results in reduction of the skin elasticity
- Other factors such as photoaging, smoking, sun exposure, hormonal changes and gravity also have an impact on the skin.
Adipose tissue
 The adipose tissue of the face is distributed roughly equally between the deep and superficial layers, divided by a superficial muscular-aponeurotic system (SMAS).
The adipose tissue of the face is distributed roughly equally between the deep and superficial layers, divided by a superficial muscular-aponeurotic system (SMAS).
The superficial portion is a continuous uneven layer interfaced with fibrous septa that connect the SMAS to the dermis.
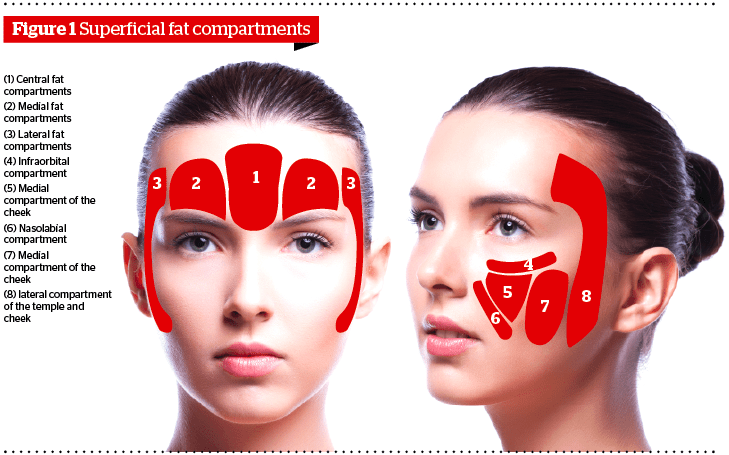
The deep layer is divided into distinct anatomical compartments delimited by ligamentous structures. It consists of three compartments in the frontal region, three in the periorbital areas, and five superficial and four deep areas in the cheeks. The intraorbital fat, the medial cheek fat, and the nasolabial fat together constitute the malar fat pad.
In the lower part of the face, the most important fat compartments in relation to aging are the jowls and mental fat compartment, and the superficial and deep mental fat, which are responsible for the rounder shape of the area4,5.
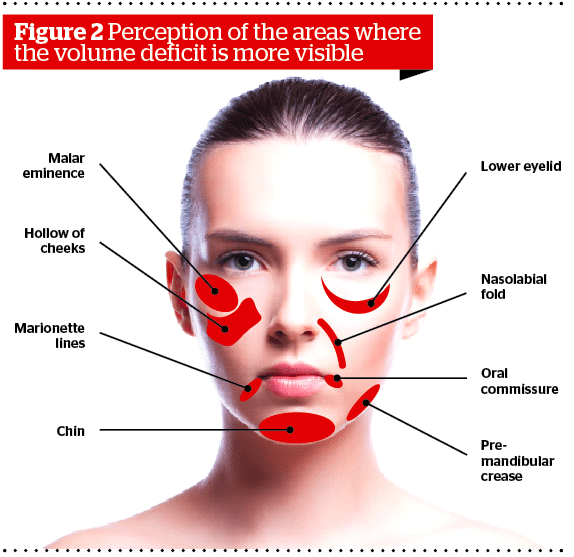
As time goes by the fat tissue is redistributed, the face loses its fullness and fat bags begin to appear as distinct and separate compartments. With age, the malar fat pad tends to slide down revealing the inferior orbital rim and contributes to the formation of naso-labial folds6.
In the author’s experience, these separate regions experience the effects of the aging process at various times in a person’s life. Therefore, the concept of separated adipose compartments explains why the face does not age as a single mass but is characterised by the changes that each of these different compartments undergoes at different times.
Some areas are subject to atrophy of the soft tissues (frontal, temporal, periorbital, perioral, jaw and chin areas) and others become hypertrophic (submandibular, nasolabial, labiomental, cheeks, infraorbital fat bags, and malar fat pads7.
Muscles and ligaments
The weakening of the malar and orbital ligaments is one of the more common events related to the aging process. One consequence is the sliding of the malar fat pad downwards and medially over the supporting ligaments of the nasolabial folds, this causes the cheeks to appear hollow. The orbital ligaments also become weaker and this contributes to the appearance of a depression below the orbits.
While some muscles get looser, others are actually tightening with age as proven by the platysma bands, permanent and deep crow’s feet, and even when the tip of the nose plunges. The most obvious signs of this can be seen in the platysma bands of the neck, which stretch from the chin to the collarbone area and become more pronounced with age. This effect can also come about in the form of permanent crow’s feet and deep-set glabella lines between the eyes.
In addition, both the major and minor zygomatic muscles, because of the undermining of the ligament and muscle connections, give the face a frowning look and contribute to accentuating the labiomental folds.
Bones
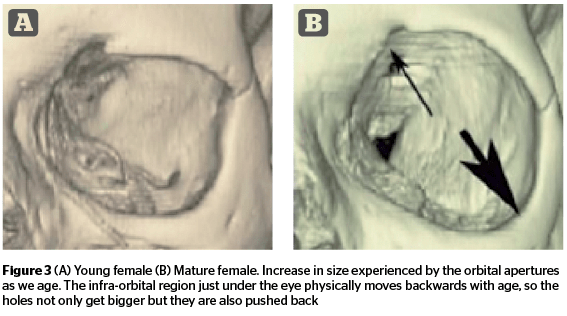
The most significant change in the facial skeleton occurs in the facial apertures, or ‘holes’ of the face, such as the nose and the eyes. The orbital apertures, or eye sockets, actually increase in size with age and the bone of the infra-orbital region below the eye physically moves backwards with age, so the holes not only get bigger but they are also pushed back8. This contributes to the lower, sunken-looking lower-eye area.
The process of bone reabsorption results in an overall reduction in bone volume. The effect of aging in the lower part of the face occurs initially in the mandibular profile. The progressive reabsorption of the jaw bone can lead to the development of a hypoplastic chin and to the formation of a front mandibular furrow9. There is also a particularly atrophic area in the front of the mandibular groove10.
Botulinum toxin
Treating the wrinkles on the upper-third of the face with Botulinum toxin type-A is now the gold standard. It works extremely well for dynamic or active lines11 and can be used in the following areas:
- Forehead (horizontal lines)
- Frown lines (vertical)
- Crow’s feet (periorbital)
- Eyebrows (arched, horizontal, gullwing). It also permits the lifting of the eyebrow
- The correction of ‘square’ jaws (hyperactive masseters) and to treat grinding teeth
- It can be used also under the nose to elevate the tip of the nose and in the nostrils (flaring nostrils)
- To stop the upper-lip elevating too much (gummy smile).
Dermal fillers
The temporal area is a small and often forgotten region of the face. It is mainly composed of the temporal muscle and the underlying adipose tissue. The aging process will generate a depression caused by the atrophy of the muscle and adipose tissue12.
In the mid-third of the face there will be a loss of skin elasticity, and a loss of volume to the deep fat of the mid-cheeks, which will cause a downward and forward descent of the malar fat pad. The result will be deeper nasolabial folds because the cheeks are more prone to relaxation.
The atrophy of bone tissue plus the increase in laxity of the orbicular ligament and zygomatic cutaneous junction ligaments will cause a descent of the malar-palpebral fat pads and an elongation in the lower eyelid. When the orbits increase in size and the jawline shrinks it makes the nasolabial folds more visible13–15.
It is possible to recreate a harmonious jawline by injecting dermal fillers into the two depression points of the pre and post jaw, but this is only creating an optical illusion. Depending on the type of filler used (density) they can be used to attenuate folds or to recreate volume where it has been lost (temporal, cheek bones, and lips) and even to reshape a nose.
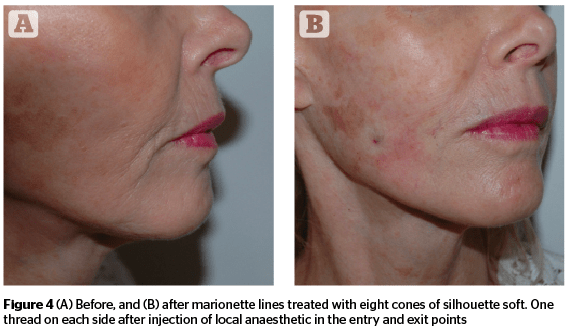
Bi-directional threadlifts
For bi-directional threadlifts, local anaesthetic injections are administered and then a small entry point is made with a 18 G needle. The thread is then inserted 5 mm under the skin into the thin fat layer following the vector that was determined before to obtain the best result. This is a technical innovation and a simple and non-invasive technique16–25. Aspects of the results that can be achieved include:
- A redefined face
- Volume restoration
- Repositioning of the cheeks
- Increased zygomatic projection
- Redefined jaw line
- Reduced wrinkles
- Lifting of the neck and eyebrows
- Tightening of the inner arms, thighs and/or abdomen.
Plasma therapy (PRP)
The Nobel Assembly at the Karolinska Institute awarded the Nobel Prize in Physiology or Medicine in 1986 jointly to Stanley Cohen and Rita Levi-Montalcini for their discoveries in 1953 of ‘growth factors’. Neural growth factor and epidermal growth factor were the first of many growth regulating signal substances to be discovered and characterized. During the last decade, several other growth factors have been isolated and characterized by different research groups.
Most reviews on this topic focus on the growth factors contained within the alpha granule of the platelet, which is released upon platelet activation. Numerous proteins are contained within the alpha-granules of platelets including:
Three isomers of platelet-derived growth factor (PDGF)
- Chemo attractive to mesenchymal stem cells and endothelial cells
- Offer differentiation for fibroblasts and osteoblasts.
Transforming growth factor (TGF)-[1 and 2]
- Promote cell mitosis
- Favours the synthesis of collagen and significantly increases type I collagen production in tendons.
Vascular endothelial growth factor (VEGF)
- Stimulates angiogenesis, chemo-attractive to osteoblasts.
Epidermal growth factor (EGF)
- Important role in the regulation of cell growth, proliferation, and differentiation by binding to its receptor EGFR
- Induces epithelial development and promotes angiogenesis
- Stimulates proliferation and differentiation of epidermis cells.
- Other proteins, including
- Platelet factor 4 (PF4)
- Interleukin (IL)-1
- Platelet-derived angiogenesis factor (PDAF)
- Platelet-derived endothelial growth factor (PDEGF)
- Epithelial cell growth factor (ECGF)
- Insulin-like growth factor (IGF)
- Osteocalcin, Osteonectin, Fibrinogen, Vitronectin, Fibronectin, and Thrombospondin (TSP).
In addition, the activated thrombocytes have on their surface a multitude of signalisation molecules: CD9, CD-W17, CD41, CD42a-d, CD51, CD-W60, CD61, CD62P, and CD63.
Platelet rich plasma is a well-documented and efficient procedure for implantology26. In sport medicine, PRP treatment has proved its efficacy even with only one session. In recent studies, injections of PRP in the face and neck for revitalization obtained good results28.
In aesthetic medicine, an Amgar study29 used biometric parameters for scientifically measurable means of assessing the results from injections of 4cc of PRP. The study also demonstrated that the effects of one PRP treatment could last for up to 10 months.
Conclusion
So now for the first time ever a synergy of treatments is available that can rejuvenate and lift the whole face without the need for surgery. While PRP will improve:
- The osteoblasts and stop/correct the bone resorption
- The tendon, ligaments and muscles
- The fibroblast and the epidermal/dermal junction.
The botulinum toxin will act on muscle contraction and eliminate active lines, the dermal fillers will correct the loss of volume, and the bi-directional threads will do the lifting and repositioning of the fat pads.