

Importance of growth factors
For a number of years, the expectations of physicians and patients in medical and surgical procedures were to improve tolerance, obtain satisfying results, and to make the treatment process easier to carry out. As a result, the use of PRP therapy began to take a prominent place in this context. The process consists of using autologous platelet extracts as a cell-repairing product. The revitalising qualities of the platelets are well known and have been used since at least 1970, in a variety of specialist areas, such as plastic surgery, rheumatology, dentistry and orthopaedics. Being an autologous product, tolerance is excellent and no serious adverse effects have been observed to date.

Figure 2 (A) Before and (B) 8 months after one session of platelet-rich plasma treatment
However, for use in hair-loss surgery, the challenge remains to evaluate the results using objective parameters. To assess the effect of PRP treatment on the skin, two studies have been published, one of which used biometric parameters (i.e. anisotropy, hydration, transepidermal water loss3 and the other using human histology4. Most clinical evaluations are based on subjective evaluations, patient satisfaction, and before and after picture evaluations. Those publications that offer objective parameters are based on biometrology or human histology. For this reason, future studies that investigate the use of PRP and hair-loss must consider objective parameters.
The process begins by taking a blood sample through an anticoagulated tube, with or without separating gel. The tubes are then centrifuged for approximately 5 minutes at 600 G (the speed and time will depend on the specific kit protocol). As a result of their density, the red cells sink in the tube, while at the upper part of the tube the plasma and platelets collect. PRP is usually referred to when a concentration of three-to-five-times normal standards has been collected.
Once injected into the dermal layer, the platelets are activated; they inflate and growth factors are released. The most important growth factors in terms of PRP for hair application are:
-
Platelet-derived growth factor (PDGF)
-
Vascular endothelial growth factor (VEGF)
-
Epidermal growth factor (EGF)
-
Insulin-like growth factor 1 (IGF-1)
-
Fibroblast growth factor (FGF)
-
Nerve growth factor (NGF).
PDGFs stimulate the growth of dermal mesenchyme. PDGF signals are involved in both epidermisÐfollicle interaction and the dermal mesenchyme interaction required for hair canal formation and the growth of dermal mesenchyme, respectively5.
VEGF belongs to a family of powerful growth factors with action on mitotic cells and the endothelial cells of blood vessels, and increases vascular permeability. The hair follicle is an avascular structure, the growth of which depends on the vessels and capillaries that form the vascular plexus in the dermal papilla. Yano et al6 identified VEGF as a significant mediator of hair follicle growth and cycling, providing the first direct evidence that improved follicle vascularisation promotes hair growth, as well as increasing follicle and hair size.
In a trial of 104 patients receiving hair transplants, Rinaldi et al7 have shown, by means of confocal microscopy, that the up-stimulation of VEGF through adenosine receptors induces significant changes in the average diameter of the scalp’s perifollicular vessels compared with placebo, and an elongation of the transplanted follicles in the anagen phase. Further studies have shown that the up-stimulation of adenosine receptors contributes to the growth of hair through direct stimulation of the production of VEGF by the dermal papilla8, 9.
EGF stimulates mitosis on epithelial cells and fibroblasts, and improves the ratio of anagen. EGF inhibits the entry in the catagen phase, promoting the anagen phase10. EGF signals control the orientation and elongation of follicles, probably attributable to its effect on the proliferation of basal keratinocytes and of cells that comprise the outer root sheath of hair. High doses of EGF can induce regression of the follicle. As proposed by Kingston et al, EGF serves as a biologic switch for entering and leaving the anagen phase11.
IGF slows down apoptosis. IGF-1 acts as a signal in mitotic different cell lines and protects cells apoptosis. IGF-1 regulates the expression of a powerful messenger cellular level, which is anti-apoptotic and capable of preventing the cell death12.
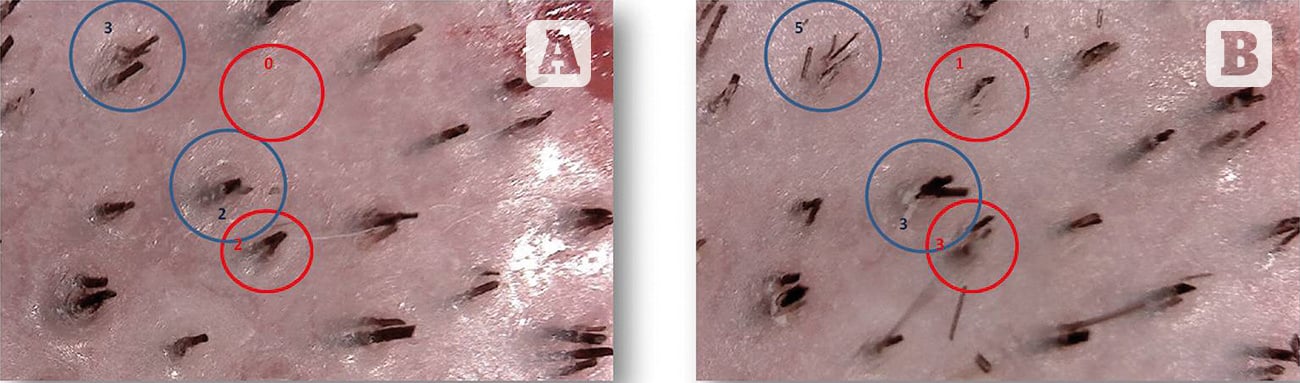
Figure 3 (A) Before and (B) 3 months after one session of platelet-rich plasma treatment
FGF stimulates the proliferation and differentiation of keratinocytes and endothelial cells. It is over-expressed in then anagen phase and then less so from stage VI of anagen13.
NGF strongly stimulates hair growth and slows down apoptosis. NGF has a modulating effect on the hair depending on the receptor with which it interacts: at the level of the outer root sheath, the complex NGF TrkA stimulates proliferation keratinocytes, while NGFj p75NTR promotes apoptosis, the regression of the follicle, and inhibits the growth of hair12.
During anagen–catagen transition, increased neuroimmune communication leads to perifollicular neurogenic inflammation, apoptosis in hair follicles, and premature catagen development. A survey of the literature on key candidates in skin–stress responses reveals that not only noradrenaline, the prominent signaling molecule of the sympathetic stress response, but also NGF, act as stress mediators. This is certainly one of the best ways in which to explain the correlation between stress and hair-loss14.

