

The soft tissue components/envelope of the nose include the skin, muscles, nerves, and different density vascular tissues. The tissue layers and fibrovascular membrane structures of the envelope in the inferior part of external nose divide into five layers: epidermis, dermis, superficial fascia, fibromuscular layer, and perichondrium. The sequence of these layers is: perichondrium/periosteum, reticular layer, fibromuscular layer, subpapillary layer, superficial fascia, and papillary layer9. Beneath the dermis lies the superficial fatty panniculus, and under the panniculus is a fibromuscular layer. Deep to the fibromuscular layer, a fatty layer encases another longitudinal fibrous sheet at scroll area that links the upper to the lower lateral cartilages (LLCs) (Figure 1). The thin, dynamic musculoaponeurotic layer of the nose is a critical structure of the nose that is difficult to visualise. Preservation of these muscles is vital to nasal function and appearance6, 7, 10, 11.
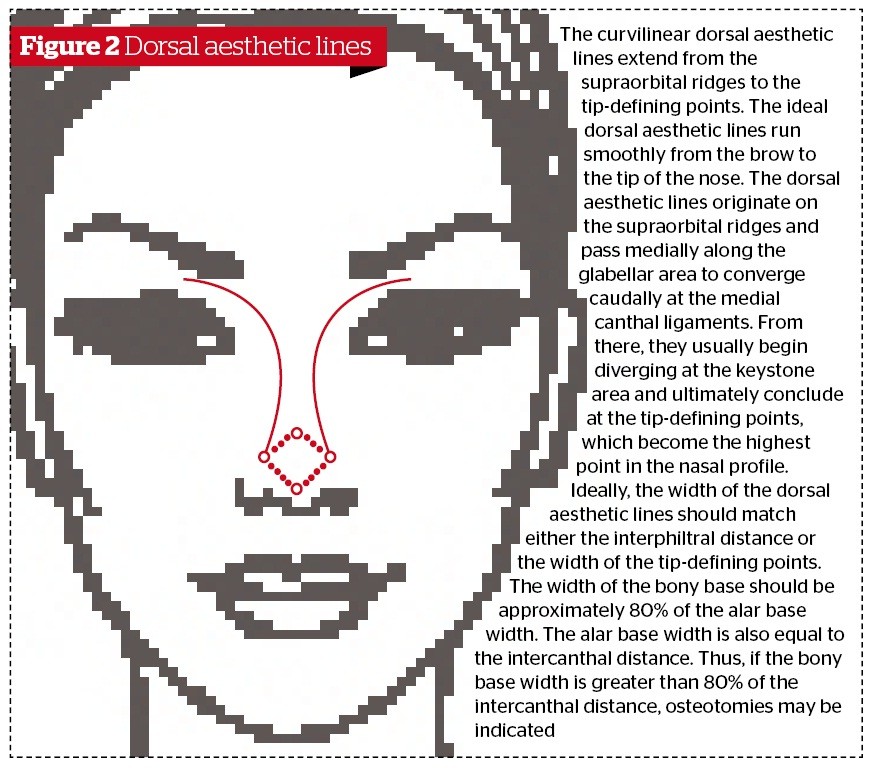
Through two divergent concave lines (nasal dorsum aesthetic lines8), which are unbroken extensions of the superciliary ridges, the nasal dorsum connects the radix with the lateral projections of the crura of the LLCs (Figure 2). The radix and supratip region have thicker soft tissue coverage, while the mid-vault area has thinner soft tissue coverage. A tip break is a place along the profile line of the nose, which continues fairly straight down to the tip, without a location above the tip where the dorsal profile line takes a little jump beyond that straight line, angling outward to surround the tip. Another feature of a nose that has good tip support is a tip-defining point. A tip-defining point simply means a place which an observer can easily identify as the location of the tip of the nose8, 12. The position of the tip-defining point is somewhat subjective, changing a little depending on ethnic characteristics, for example. To achieve a balanced dorsal profile and dorsum with a supratip break, it is necessary to respect differential soft tissue thickness, tip–dorsal stabilisation and supporting connective ligaments, which mandate a frame with a slightly deeper nasion and tip projection beyond the dorsum7, 10–13. Over-reduction of the dorsum causes a change in the orbital–nasal relationship, with a flattening of the midface, which patients feel leads to an unfavourable change in the appearance of the eyes. From an aesthetic standpoint, the area from the nasal bridge to nasal tip should be aligned and straight14, 15.
Rhinoplasty complications
Primary rhinoplasty surgery can be associated with many risks, the main complications of which are postoperative deformities, often requiring revision rhinoplasty surgery. Clinical manifestations of rhinoplasty complications and side-effects may be classified as functional and aesthetic, or a combination of both. To solve these problems, a number of technical methods have been proposed4–18. From the variety of complications described, it is imperative that more care and attention are paid to surgical techniques for reconstruction of nasal tip projection and dorsal aesthetic lines in patients with a prominent hump.
Internal nasal valve incompetence (INVI) occurs in conjunction with the inverted-V deformity (disruption of the dorsal aesthetic lines) caused by a collapse of the ULCs after dorsal humpectomy, which renders the caudal edge of the nasal bones visible. This dual complication can be prevented and corrected during dorsal component hump reduction by avoiding excessive resection of the ULC as compared with the septum (mid-vault area), and by placement of spreader grafts19.
The nasal tip presents an exceptional challenge owing to its mobility, and tip-plasty is most the difficult aspect of aesthetic rhinoplasty10–15. Sacrifice of tip support and projection by the healing forces is one of the most common surgical errors. During dorsal hump reduction, if the K-area is disrupted and not aligned with the nasal bridge, it may act as a pivot point; downward and inward rotation of the anterior septal cartilage then becomes possible, disproportionately widening the nasal base and resulting in an unnatural appearance of the dorsal aesthetic lines. This protuberant piece of cartilage can then appear as a pollybeak deformation or suptratip deformity. A nose with a pollybeak shows protuberance with a rounded downward pointing tip, and with fullness of the supratip region — much like that of a parrot’s beak. Excess scar tissue in the area of the dorsal–septal cartilage or supratip region can cause a protuberant deformity, becoming apparent once post-surgical swelling has subsided. It is more likely in patients with thick skin. For the prevention of this deformity, every attempt should be made to maintain adequate tip support through columellar struts or suturing techniques. Suturing the supratip subcutaneous tissues to the caudal dorsum and scroll areas eliminates dead space and formation of deep scar tissues, preserving the functional and aesthetic anatomy of the nose10–14.

