


Kai Kaye and Gabriela Casabona discuss how three-dimensional ageing must be considered when injecting the face in order to achieve satisfactory results in facial rejuvenation
Volume loss of both bony and soft tissue results in loss of projection and subsequent skin ptosis, leading towards a concave facial contour with deepened nasolabial folds and mid-cheek grooves, resulting in changes in the double ogee shape of a youthful facial contour towards an aged and exhausted appearance1.
Facial recontouring with autologous fat grafting has become widely accepted for facial rejuvenation either as a stand-alone procedure or in combination with surgical lifting techniques since its introduction by Coleman. Since then multiple techniques to optimize fat grafting have been suggested, such as structural fat grafting (Coleman technique), the 3M3L technique, and nanofat grafting2–4. Rohrich et al. first focused on facial fat distribution, showing that facial fat is highly compartmented consisting of multiple layers of fat compartments, including both superficial and deep fat5–9.

Figure 1 (A) Temples Before, (B) after. Injected with microfat, intramuscular and prefascial , 12 cc per side
The facial contour is defined by these fat compartments, which change in a variety of ways during ageing, and, therefore, an augmentation technique taking into account the physiologic changes occurring at these sites should be developed to avoid a generic look after facial fat grafting10,11.
Many competing studies show that there is no consensus so far in the literature regarding the techniques and the injection site for fat grafting12–15.
In the following article, the authors want to outline their personal, area-based approach towards pan-facial rejuvenation based on an algorithm taking into account the main aesthetic goal, type of fat, layers to be restored, and desired aesthetic effect.
Area 1: Temples
The temples are one of the first areas to age and its deflation, due to a loss of volume in the fat compartments, leads not only to a descent of the brow and the lateral area of the face but also, in severe hollow temple patients, to a skeletonized look and loss of contour in the anterior temples. Our goal is not only to restore volume into the deep fat compartments to recontour the area but also to augment the projection and, therefore, provide support for the lateral eyebrow and lateral cheek. Nanofat is used in the area overlying the venous plexus to achieve dermal rejuvenation via a stromal vascular fraction (SVF) effect.
- Type of fat: microfat and nanofat
- Layer injected: posterior temple (behind hairline) deep layer microfat/anterior temple microfat deep compartments and intramuscular and nanofat superficial compartments.
- Aesthetic effect: lifting and revolumising of the lateral brow, lifting of the lower lateral temple/lateral orbital region.
Area 2: Midface/malar
Deflation of the midface/malar areas occurs quite early during the ageing process. As the volume loss in combination with the progressive loss of bony support by the inferior orbital rim leads quickly to a lack of support of the lower eyelid, even young patients often complain about having a ‘tired’ look. Re-volumising the SOOF and restoring support for the lower eyelid is one of the main goals, as well as recontouring of the zygomatic bone to augment projection and to achieve a lifting to the lateral face
- Type of fat: microfat
- Layer injected: deep compartments anterior and lateral cheek, SOOF
- Aesthetic effect: better contour of the cheek/malar and smooth transition into the lower face, less sunken and deflated lower eyelid with short and re-volumised lid-cheek junction and a more ‘rested’ look.
Area 3: Mandible/gonial angle
The mandibles not only define the framework of a masculine look in men but also provide strut-like tension support for the overlying facial skin in both sexes. An under projecting mandible does not provide this strut-like support anymore and leads to the early formation of jowls.
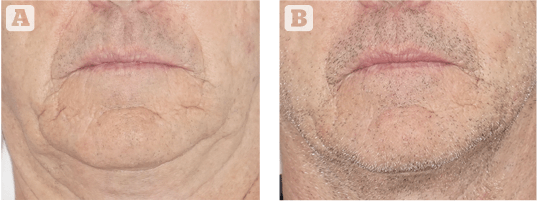
Figure 2 (A) Perioral before, and (B) after. SNIF intradermal nanofat injection perioral 5 cc total, microfat upper/lower lips 2 ml each, 2 cc marionette fold, 3 cc nasolabial groove per side
According to Shaw et al. the gonial angle and the mental protuberance of the body start losing projection from age 25 years onwards; therefore, restoration of volume and reconstitution of the angle should be considered early in both sexes as an approach to delay the ageing related changes described above16,17.
- Type of fat: microfat
- Layer injected: deep to SMAS/Periosteal
- Aesthetic effect: better contour and definition of the jaw. Better posterior projection of the gonial angle and anterior projection of chin/mental protuberance to augment projection of the mandible, to enhance the cervico-mental angle and to provide a lifting effect for the anterior neck.
Area 4: Periorbital/brow
In the authors’ opinion the brow and periorbital area form an aesthetic unit that should be addressed conjunctively, as their visual connection defines the frame of any beautiful eye.
Progressive descent of the brow caused by laxity of the forehead skin in combination with deflation of the ROOF during the ageing process leads to a heavy upper-eyelid and patients often complain about looking ‘sad’. Atrophy of the superficial portion of the ROOF underlying the lid crease leads to an augmentation of visible upper eyelid height (doll eye effect). Age-related atrophy of the SOOF augments the visible lower lid length and deepens the lid-cheek junction, and subsequent exposure of the underlying structures like fat compartments and canthal ligaments results in the skeletonisation of the infraorbital area.
Revoluminisation of lateral eyebrow fullness and reprojection of the eyebrow shape are the key goals when treating this area; as well as the reduction of upper-lid height, correction of lower lid skeletonisation, and treatment of dark circles.
- Type of fat: microfat and nanofat
- Layer injected: brow and deep forehead layers microfat on the periosteum, upper eyelid microfat in ROOF and nanofat superficial in the upper eyelid crease, lower eyelid microfat under the orbicularis oculi muscle and nanofat over the orbicularis oculi to achieve dermal rejuvenation via an SVF effect
- Aesthetic effect: better contour of the brow, restoration of lateral fullness with brow elevation, correction of the skeletonisation effect, correction of eyelid height and lid /cheek junction, correction of dark circles.
Area 5: Perioral/lips
In much the same way as the periorbital area should not be addressed separately from the brow; the perioral area forms an equally strong aesthetic unit with the lips. Structures like the philtrum, the white roll and the vermillion support the lip and define its youthful shape.

Figure 3 (A) Panfacial before, and (B) after. Microfat chin 7 cc total, mandibular 8 cc, gonial angle 6 cc, upper/lower lips 2 cc each, philtrum/supraoral 6 cc, malar 6 cc ,infraorbital 2 cc, lat brow 2 cc, temples 6 cc per side
From the mid-twenties onwards the maxillary bone begins to lose projection and with further advance of the ageing process the deep submuscular fat compartments also lose volume resulting in a loss of support for the anatomic structures mentioned above.
The lip becomes straight, loses the cupid bow shape and becomes inverted. In cases with severe deflation and loss of volume in the subcutaneous layer, the patient often complains about the ‘bar code’ appearance of the upper lip. The restoration of support and recreation of a youthful shape is one principal goal in this area, as well as conservative volume restoration and correction of dermal wrinkles.
- Type of fat: microfat and nanofat
- Layer injected: perioral/philtrum deep compartments — microfat, intramuscular lips — microfat, white roll — nanofat, upper lip superficial subdermal layers — nanofat
- Aesthetic effect: better contour of the lip and proportions, lip eversion, smoother skin and wrinkles around the mouth.
Area 6: Piriformis fossa/nasolabial/deep cheeks
The nasolabial fold was one of the first clinical indications in the advent of volume restoration with injectable fillers.
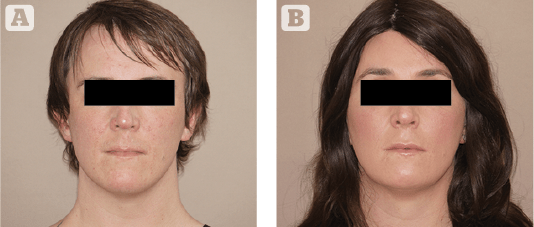
Figure 4 (A) Panfacial transgender before, and (B) after. Microfat forehead 7 cc, chin 4 cc total, mandibular 10 cc, upper/lower lips 2 cc each, philtrum/supraoral 4 cc, malar 8 cc ,infraorbital 3 cc, lat brow 4 cc, temples 8 cc per side
At that time, the anatomy of the deep and superficial fat compartments of the face was not yet fully described, and treatments with injectables concentrated on linear filling along this fold. The formation of this fold and its subsequent deepening during the ageing process is the result of a loss of soft tissue volume and bone projection not only along the line but in all adjacent areas; therefore, it should be treated as a unit. The widening of the piriform fossa due to bone resorption of the maxillae leads to an inwards rotation and depression of the soft tissues on both sides of the nose, a loss of support of the upper lip/philtrum area and loss of support of the nasal base. Subsequently, the support to the lateral deep cheek compartments is diminished, which leads to the deflation of the deep cheek fat compartments to a downwards/inwards sagging of the cheek, further enhancing the development from a depression into a fold.
Patients often complain of a ‘sad’ or ‘aged’ look, and the goal in this area is the restoration of a smooth transition between the cheek and the perioral area.
- Type of fat: microfat
- Layer injected: piriform fossa, deep cheek fat compartments periosteal /deep, spina nasalis/philtrum periosteal/ submuscular under orbicularis oris
- Aesthetic effect: Smooth transition between perioral area and cheek with volumising of perioral area, re-projection and eversion of the lip with correction of gummy smile, enhanced support of the nasal base.
Processing and harvesting
Different approaches for processing microfat to nanofat and intradermal injection are described in the literature. The authors use manual destruction of the adipocytes through filters of descending diameters or by multiples passages through a 3-way–tab while closing the tab progressively.
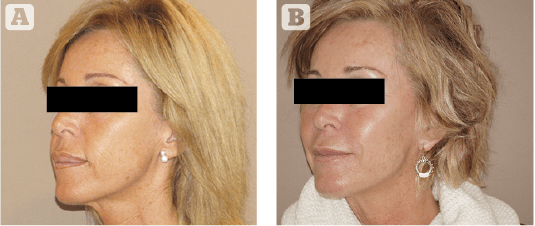
Figure 5 (A) Cheek/malar before, and (B) after. Microfat forehead 10 cc, mandibular 5cc, chin 4 cc, upper/lower lips 2 cc each, philtrum/supraoral 4 cc, malar 6 cc, infraorbital 3 cc, lateral brow 2 cc, temples 8 cc per side
Harvesting the microfat is performed either using an inside sharp, multihole 1.8 mm cannula for smaller volumes after injection with tumescence fluid (modified Klein’s solution, no sodium bicarbonate, lidocaine only in cases without GA); for larger volumes (more than 50 cc) a waterjet system for lipocollection is used (Bodyjet Eco, HumanMed AG).
Safety
As the success of any fat grafting procedure depends on a variety of factors, especially on the careful handling and even distribution of the fat aliquots, the surgeon should gather enough experience with single zone, small volume approaches before performing large volume, pan-facial single treatments to avoid the multiplicator effect for complications.

Figure 6 (A) Periorbital before, and (B) after. Microfat, 4 cc infraorbital, 3 cc lateral brow
To avoid intravascular injections, the injection should be performed with a retrograde movement of the cannula, and the injector should avoid placing a degree of pressure on the plunger. Vascular anatomy should be visualised prior to injections, and injection pathways should be perpendicular to large vessels, not parallel, to minimise the possibility of vascular canulization. In areas with large diameter vessels at the surface, digital compression of the main vessel minimises flow and vessel diameter.
Conclusion
The overall goal of pan-facial rejuvenation using a combination of micro and nanofat in a holistic, anatomy-based approach is not only to restore a youthfully shaped face but also to create beauty through enhanced proportions and to recreate the natural glow and aspect of what we find in younger skin, resulting in a true 3-dimensional regeneration concept.
Declaration of interest None
Figures 1–6 © Dr Kaye
References:
- Hopping SB, Joshi AS, Tanna N, Janjanin S. Volumetric facelift: Evaluation of rhytidectomy with alloplastic augmentation. Ann Otol Rhinol Laryngol. 2010;119:174–180
- Coleman SR. Facial augmentation with structural fat grafting. Clin Plast Surg. 2006;33:567–577
- Xie Y, Zheng DN, Li QF, et al. An integrated fat grafting technique for cosmetic facial contouring. J Plast Reconstr Aesthet Surg. 2010;63:270–276.
- Tonnard P, Verpaele A, Peeters G, Hamdi M, Cornelissen M, Declercq H. Nanofat grafting: Basic research and clinical applications. Plast Reconstr Surg. 2013 Oct;132(4):1017-26.
- Rohrich RJ, Pessa JE. The fat compartments of the face: Anatomy and clinical implications for cosmetic surgery. Plast Reconstr Surg. 2007;119:2219–2227; discussion 2228
- Rohrich RJ, Pessa JE. The anatomy and clinical implications of perioral submuscular fat. Plast Reconstr Surg. 2009;124:266–271
- Rohrich RJ, Arbique GM, Wong C, Brown S, Pessa JE. The anatomy of suborbicularis fat: Implications for periorbital rejuvenation. Plast Reconstr Surg. 2009; 124: 946–951
- Wan D, Amirlak B, Giessler P, et al. The differing adipocyte morphologies of deep versus superficial midfacial fat compartments: A cadaveric study. Plast Reconstr Surg. 2014;133:615e–622e
- O’Brien JX, Ashton MW, Rozen WM, Ross R, Mendelson BC. New perspectives on the surgical anatomy and nomenclature of the temporal region: Literature review and dissection study. Plast Reconstr Surg. 2013;132:461e–463e.
- Gierloff M, Stöhring C, Buder T, Gassling V, A.il Y, Wiltfang J. Aging changes of the midfacial fat compartments: A computed tomographic study. Plast Reconstr Surg. 2012;129:263–273
- Rohrich RJ, Pessa JE, Ristow B. The youthful cheek and the deep medial fat compartment. Plast Reconstr Surg. 2008;121:2107–2112.
- Stallworth CL, Wang TD. Fat grafting of the midface. Facial Plast Surg. 2010;26:369–375.
- Sadick NS, Manhas-Bhutani S, Krueger N. A novel approach to structural facial volume replacement. Aesthetic Plast Surg. 2013;37:266–276
- Kaye KO, Schaller HE, Jaminet P, Gonser P. The PAVE (peeling-assisted volume-enhancing) lift: A retrospective 6-year clinical analysis of a combined approach for facial rejuvenation.J Plast Reconstr Aesthet Surg. 2016 Aug;69(8):1128-33
- Wang W, Xie Y, Huang RL, Zhou J, Tanja H, Zhao P, Cheng C, Zhou S, Pu LL, Li Q. Facial Contouring by Targeted Restoration of Facial Fat Compartment Volume: The Midface. Plast Reconstr Surg. 2017; 139(3): 563-572
- Shaw RB, Jr, Katzel EB, Koltz PF, et al. Aging of the facial skeleton: aesthetic implications and rejuvenation strategies. Plast Reconstr Surg. 2011;127(1):374–383
- Shaw RB, Jr, Katzel EB, Koltz PF, et al. Aging of the mandible and its aesthetic implications. Plast Reconstr Surg. 2010;125(1):332–342






{kind=link}