


Monica Boen, Monique Wilson, and Jeffrey Hsu discuss their approach, including sclerotherapy, fillers, and laser resurfacing for a visually important but often overlooked part of the body
The hands are the second most perceivable part of the body after the face1, making aesthetically appealing hands an integral part of maintaining a youthful and healthy appearance. While many patients now undergo facial rejuvenation procedures, the hands can reveal a patient’s true age. Ageing of the hands is a result of both intrinsic and extrinsic factors, such as increased skin laxity, atrophy of the skin and subcutaneous fat, chronic photodamage, and environmental factors including pollution and smoking2. The dorsum of the hands in particular receives substantial exposure to ultraviolet radiation and can be one of the first areas on the body to manifest photodamage. Common reasons patients seek restorative treatments for their hands include dyspigmentation, loss of subcutaneous fat, and prominent veins. There are several new minimally invasive procedures and technologies to improve the appearance of the hands, and the authors suggest a unique combination of treatments to restore hands to their former beauty.
There are three main targets in hand rejuvenation: enlarged veins, atrophy, and photodamage. The authors use a three-step method that includes sclerotherapy, volume restoration, and laser resurfacing to address these issues and improve the appearance of the hands.
Sclerotherapy
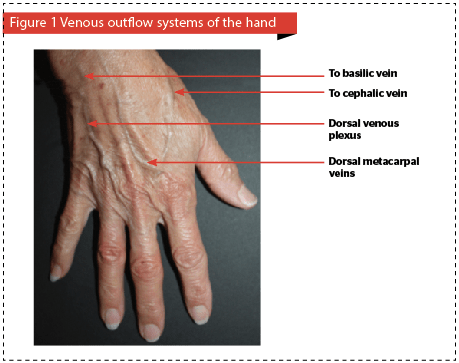 Sclerotherapy is used to treat the enlarged veins on the dorsal hand. The venous outflow system in the hands is composed of three communicating systems: the superficial palmar veins, deep palmar veins, and the dorsal veins (Figure 1). Therefore, when one system is eliminated by sclerotherapy, there are still two other outflow systems in the hand to aid in venous drainage. The dorsal veins, composed of the metacarpal and dorsal venous veins, are the predominant source for the enlarged and tortuous veins of the hands, and are the most common veins treated with sclerotherapy. Caution must be practiced when performing sclerotherapy on the hands to prevent venous obstruction in the hand and upper extremity due to occlusion of the basilic vein, median cubital vein of the forearm, and cephalic vein. Occlusion of the cephalic vein can be prevented by avoiding injection at the dorsal base of the thumb. Relative contraindications to sclerotherapy in the hands include carpal tunnel syndrome, history of hand surgery, presence of dialysis shunts, and chronic myalgia or arthralgia in the hands.
Sclerotherapy is used to treat the enlarged veins on the dorsal hand. The venous outflow system in the hands is composed of three communicating systems: the superficial palmar veins, deep palmar veins, and the dorsal veins (Figure 1). Therefore, when one system is eliminated by sclerotherapy, there are still two other outflow systems in the hand to aid in venous drainage. The dorsal veins, composed of the metacarpal and dorsal venous veins, are the predominant source for the enlarged and tortuous veins of the hands, and are the most common veins treated with sclerotherapy. Caution must be practiced when performing sclerotherapy on the hands to prevent venous obstruction in the hand and upper extremity due to occlusion of the basilic vein, median cubital vein of the forearm, and cephalic vein. Occlusion of the cephalic vein can be prevented by avoiding injection at the dorsal base of the thumb. Relative contraindications to sclerotherapy in the hands include carpal tunnel syndrome, history of hand surgery, presence of dialysis shunts, and chronic myalgia or arthralgia in the hands.
The authors prefer foam sclerotherapy over liquid sclerotherapy for the treatment of the prominent veins of the dorsal hand because of improved efficacy and fewer adverse events due to the need for a lower concentration of sclerosant3. While foam sclerotherapy has mainly been reported in the literature for use in treating lower extremity veins, in the authors’ experience it is also safe and efficacious for use in the dorsal hands4. The first step in performing foam sclerotherapy consists of mixing detergent sclerosing solutions, such as sodium tetradecyl sulfate (STS) or polidocanol (POL), with room air or carbon dioxide in a 1 : 4 ratio3,5,6. For example, 1 ml of POL and 4 ml of room air in two separate syringes are connected by a female luer lock connector and mixed back and forth 10 times to produce 5 ml of foam. The authors preferred sclerosing solution is POL due to fewer adverse events than STS7. In a multi-center study by Rabe and colleagues, 316 patients with reticular veins and telangiectasias were randomized to receive POL, STS, or placebo, and POL showed equal efficacy to STS, but had a better safety profile8.
After the foam sclerosant is prepared, a tourniquet is applied around the forearm to dilate the distal vessels, and 3–5 cc of foamed polidocanol (0.5–1%) per hand is then injected into the dorsal metacarpal and dorsal venous plexus veins. The injections are performed distal to proximal. Afterwards, compression gloves or ace wraps are applied for 1 week to mitigate the expected swelling of the hands. Coagulum formation is common and has been reported in the literature3. Drainage with an 18-gauge needle in 2–4 weeks leads to rapid resolution of the coagulum. Adverse events include bruising, telangiectatic matting, hyperpigmentation, and, rarely, necrosis5. Nonetheless, this procedure is tolerated well by patients.
 Volume restoration with calcium hydroxylapatite
Volume restoration with calcium hydroxylapatite

Several weeks after sclerotherapy of the enlarged veins of the dorsal hand, volume restoration can be performed with calcium hydroxylapatite (CaHA). This biocompatible injectable filler is composed of calcium hydroxylapatite microspheres suspended in an aqueous carrier gel. It is the only FDA-approved cosmetic filler for soft tissue augmentation in the dorsum of the hands and retains its effect for up to 2 years9. Other off label cosmetic fillers that have been used for hand restoration include hyaluronic acid (HA), poly-l-lactic acid (PLLA), and autologous fat. HA requires a greater amount of product than CaHA, carries a risk of Tyndall effect, and has a shorter duration of 6 to 12 months, which can make HA a more expensive option for patients10,11. PLLA, a biocompatible synthetic filler, requires several sessions to achieve the desired effect, and autologous fat transfer is a time consuming procedure with the potential for more complications than cosmetic fillers11. Ultimately, the type of product selected for volume restoration of the hands will depend on these considerations, as well as patient preference.
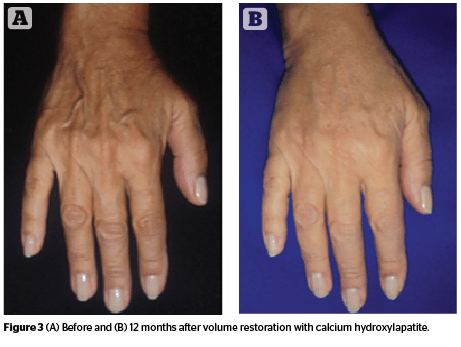
While there are several options for dorsal hand augmentation, the authors’ preference is CaHA for its long lasting effect and the need for only one treatment for excellent cosmetic results. The authors typically use 1.5 cc of CaHA mixed with 1.0 cc of 2% lidocaine for each hand. The amount of product used in each hand will depend on the severity of volume loss, but should not exceed more than 3 ml per hand12. The injection is performed with a 27 gauge needle and bruising is very rare with this technique. During the injection, the skin is pinched and lifted in six areas on the dorsum of the hand to allow for easier injection into the suprafascial plane (Figure 2). The dorsum of the hand has three compartmentalized fatty laminae that are separated by fascia13. Unlike the deeper layers of the fatty laminae, the superficial fatty lamina lacks dorsal veins, nerves, or extensor tendons, which makes it an ideal plane for the injection of cosmetic fillers. A post-injection massage is then performed to ensure even distribution of the product14. Swelling and mild soreness in the area for one week is an expected side-effect. While rare, potential long-term complications of CaHA volume restoration on the hands includes permanent swelling, paresthesias, and foreign body granuloma formation15. Most patients tolerate this procedure very well and are pleased with the long-lasting results (Figure 3).
 Several studies have shown the efficacy and safety of CaHA for rejuvenation of the dorsal hand14, 16, 17. Sadick demonstrated that volume restoration of the dorsal hands with CaHA has sustained durability and patient satisfaction after 52 weeks14. A method to evaluate the amount of volume restoration needed in the dorsal hands is the Merz Hand Grading Scale (MHGS). It is a five-point assessment tool that ranges from a score of 0 in a youthful hand where there is no loss of fatty tissue to a score of 4 consisting of severe loss of fatty tissue and marked visibility of tendons and veins19. The MHGS has been validated to assess the effectiveness of CaHA treatment for hand augmentation and, while mostly utilized in research studies, it can also be used by clinicians to evaluate the degree of improvement after cosmetic filler therapy12.
Several studies have shown the efficacy and safety of CaHA for rejuvenation of the dorsal hand14, 16, 17. Sadick demonstrated that volume restoration of the dorsal hands with CaHA has sustained durability and patient satisfaction after 52 weeks14. A method to evaluate the amount of volume restoration needed in the dorsal hands is the Merz Hand Grading Scale (MHGS). It is a five-point assessment tool that ranges from a score of 0 in a youthful hand where there is no loss of fatty tissue to a score of 4 consisting of severe loss of fatty tissue and marked visibility of tendons and veins19. The MHGS has been validated to assess the effectiveness of CaHA treatment for hand augmentation and, while mostly utilized in research studies, it can also be used by clinicians to evaluate the degree of improvement after cosmetic filler therapy12.
Laser resurfacing
The final step in hand rejuvenation involves laser resurfacing to improve skin texture and diminish the appearance of solar lentigines and keratoses. Traditional laser resurfacing with ablative carbon dioxide or erbium yttrium aluminum garnet lasers requires a significant recovery time and is fraught with the potential for dyschromia and scarring. In the past decade, fractional non-ablative lasers have been developed that allow for more targeted energy delivery into the epidermis and dermis. The 1550 nm erbium-doped fiber laser (EDF) and 1927 nm thulium fiber laser (TFL) are fractional non-ablative lasers (Fraxel Re:store DUAL, Solta Medical, Hayward, CA) that deliver energy to only a fraction of the skin in microthermal treatment zones (MTZ)20. The use of MTZ allows more rapid healing than the traditional ablative lasers. The EDF can target the dermis to a depth from 400–1,100 μm, thus allowing for improvement in skin texture, rhytides, and dyspigmentation21. The TFL is an excellent complement to the EDF as it targets the superficial epidermis with a penetration depth of about 300 μm and allows treatment of superficial epidermal lentigines and keratoses.
 The EDF and TFL have been shown to improve photodamage with minimal downtime. Wanner and colleagues treated 50 patients with facial and non-facial photodamage using the EDF with three successive treatments spaced 3–4 weeks apart and results showed a 51–75% improvement in photodamage after 9 months in 73% of facial skin and 53% of non-facial treated skin22. A pilot study by Polder and colleagues demonstrated a 51–75% improvement in non-facial photodamage in a majority of patients after three treatments with the TFL performed at 3–4 week intervals at 1 month follow-up visit23. Six bilateral dorsal hands were treated in this study, and 4 out of 6 dorsal hands had at least 51–75% improvement in photodamage. Adverse events in both studies were minimal and included erythema and mild edema, and there were no prolonged pigmentary changes or scarring. Intense pulsed light and Q-switched lasers can also be used as adjunctive treatments with EDF and TFL in some patients to further target solar lentigos or erythema10.
The EDF and TFL have been shown to improve photodamage with minimal downtime. Wanner and colleagues treated 50 patients with facial and non-facial photodamage using the EDF with three successive treatments spaced 3–4 weeks apart and results showed a 51–75% improvement in photodamage after 9 months in 73% of facial skin and 53% of non-facial treated skin22. A pilot study by Polder and colleagues demonstrated a 51–75% improvement in non-facial photodamage in a majority of patients after three treatments with the TFL performed at 3–4 week intervals at 1 month follow-up visit23. Six bilateral dorsal hands were treated in this study, and 4 out of 6 dorsal hands had at least 51–75% improvement in photodamage. Adverse events in both studies were minimal and included erythema and mild edema, and there were no prolonged pigmentary changes or scarring. Intense pulsed light and Q-switched lasers can also be used as adjunctive treatments with EDF and TFL in some patients to further target solar lentigos or erythema10.
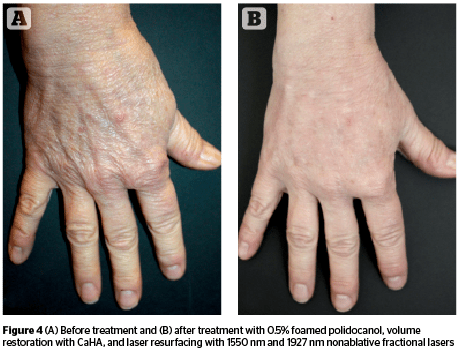
It is important to keep in mind the inherent differences between skin on the face and dorsal hands. The skin is thinner on the dorsum of the hand than the face, and there are fewer pilosebaceous units10. Therefore, lower energy settings and extra caution must be used when performing laser resurfacing on the dorsal hands. The laser settings of the EDF and TFL will vary depending on the age of the patient, degree of photodamage, and Fitzpatrick skin type. The EDF and TFL are used on the same day to safely treat the photodamage and rhytides on the dorsal hands. Usually 1–2 treatments are needed (Figure 4). During the first week, patients can experience some erythema and mild edema, but scarring and dyspigmentation are rare. Laser resurfacing may be performed on the same day as CaHA filler, taking advantage of the anesthetic effect of the CaHA mixture.
Conclusion
Combination therapies for hand rejuvenation are increasingly common, but there are few studies in the literature evaluating their optimal use10. Foam sclerotherapy has been used safely and successfully for the dorsal hand veins, and several studies have shown that CaHA filler has a safe and durable effect for volume restoration of the hands3, 6, 10. In addition, several laser and light based devices can be used to target photodamage and skin laxity6. The authors’ three-step combination method is a simple approach to creating a youthful appearance of the hands.





