

Wrinkles
Peeling treatments are not indicated for all wrinkles or depressions. For nasolabial folds, for instance, the use of fillers on the medium third of the face in order to revolumise would most likely be a better approach. On the other hand, it would be wrong to say that the facial ageing process is only casued by a loss of volume; many patients do not require volume repositioning, as they mainly present ‘superficial’ skin-level changes. These are good candidates for other treatments, such as chemical peels.
Metaphorically speaking, it can be said that a pillow loses its shape because the sponge inside becomes less malleable, less thick or because the fabric on the outside loses elasticity. Similarly, chemical peels are indicated for situations in which the outer ‘fabric’ is aged. In those patients for whom there is a need to revolumise and treat the cutaneous surface, the treatment will preferably start with volume repositioning using fillers or lipofilling. Some wrinkles, such as lip wrinkles — particularly if they are deep — may be primarily corrected with peeling to avoid the risk of hypercorrection if too much filler is used.
Static wrinkles respond better to chemical peels, while dynamic wrinkles respond better to botulinum toxin or fillers. Occasionally, a combination of both static and dynamic wrinkles are present and both techniques are required. In such cases, the author’s preferred option is to carry out muscle relaxation, followed by a chemical peel 3–4 weeks later.
Chemical peels are a good option when the ageing process is disseminated, that is, when it is not limited to a specific facial area, as they provide complete full-facial rejuvenation. They are not primarily indicated for isolated wrinkles, even if they are deep. In these cases, another method should be considered, such as soft tissue fillers.
Cervicofacial lifting and blepharoplasty remove excessive skin and may improve the look of certain wrinkles, even though they are not primarily indicated for wrinkle reduction. Whenever a patient is referred to one of these surgical procedures in conjunction with a peeling treatment, as a rule the author would perform the peeling first to allow for a more visible and immediate rejuvenation effect. This will also ‘clear the ground’ and the following surgery will then be simpler and more effective.
Medium-depth peels treat textural changes as well as superficial wrinkles, while deep peels are indicated for the treatment of installed deep wrinkles. In the author’s opinion, superficial peels are of little interest in the primary treatment of wrinkles, and they are not used for that purpose by the author.
With all this in mind, it is clear that patient selection is not always a straightforward process and calls for sensible judgement. A chemical peel must be seen as a treatment with its own specific indications and part of an assortment of techniques and technologies available to aesthetic surgery and medicine. Good patient selection is paramount when performing chemical peels. The ideal candidate for a medium or deep peels is a healthy person, skin phototype II–III, with moderate to severe wrinkles, localised or settled on the entire face. Treatment expectations should be managed through patient discussion.
Medium-depth peels
Medium-depth peels are relatively well tolerated treatments, with low complication rates, requiring approximately 4–7 days of social downtime. The process invariably involves spontaneous skin desquamation, and both its evolution and results are fairly predictable. They offer a good cost‑to‑benefit ratio, are fast to perform, and have few contraindications. Solar exposure is allowed 3–4 weeks later and serial treatments can be set approximately 4 weeks apart. Patients eventually respond well to this kind of treatment.
Trichloroacetic acid (TCA) is perhaps the most frequently used agent for a medium peel. The author has been using this particular agent for over 10 years. It is a well-known, widely used, safe, and easy-to-obtain agent. It can be applied in a range of concentrations; however, maximum values of 35–40% are not usually exceeded when used as an isolated agent. It can be used in lower concentrations with equivalent power, following a superficial peel (using glycolic acid — which is an alpha hydroxy acid — or salicylic acid — which is a beta hydroxy acid) or a microdermabrasion using a dermaroller or equivalent device.
The protocol used by many practitioners is fairly similar when compared and relatively simple to reproduce. The peel is applied by cosmetic units, to gradually increase the patient’s tolerance, until the intended end point is reached, which is a whitish almost opaque frosting, with some erythema.
Oedema may appear on the first day and by the second day the skin should start to darken; the patient may report a feeling of skin tightening. On the third day, desquamation will take place, starting at the perioral area (where most facial movement is experienced) and gradually extending to the rest of the face. Re‑epithelisation will be complete by the fifth day (Figure 1).
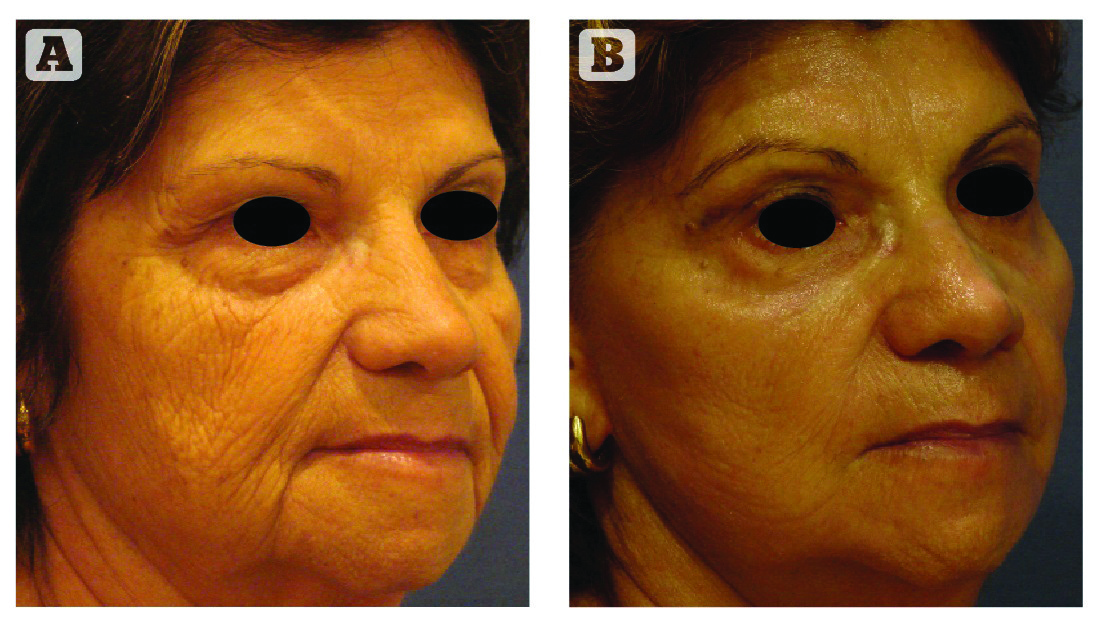
Figure 2 Patient (A) before and (B) 8 weeks after face lift and peri-oral (upper lip, inferior lip and chin) deep peel
TCA may cause discomfort or even pain, and therefore the use of troncular anaesthesia blocks or intravenous sedation must always be taken into consideration for higher concentrations or less tolerant patients. The discomfort will start to wear off in approximately 15 minutes as the frosting disappears. Based on the author’s experience, different patients will demonstrate a varied tolerance towards the peels. Some young patients with thin skin will tolerate high concentrations, while a 15% TCA may be challenging for some older patients presenting with severe elastosis. Higher phototypes and oily skins may be less tolerant, as higher concentrations and longer agent exposure is normally required.
In the author’s clinical practice, he often combines a medium peel with a surgical procedure, such as a blepharoplasty or a cervicofacial lifting, durinf the same operating time (Figure 2).
Deep peels
The deep peel is, according to many practitioners, the most powerful facial rejuvenation method available. Results are long-lasting and some consider it to be a ‘once in a lifetime’ procedure. Owing to its outstanding efficacy, it’s a technique that practitioners often feel tempted to perform.
Many doctors use a range of different substances and formulae to perform deep peels. Most solutions comprise a combination of different concentrations of phenol, also known as carbolic acid; croton oil, oil obtained from plant seeds; and lesser quantities of other substances such as septisol, resorcinol, salicylic acid, and excipients. Modern formulae tend to have a lower quantity of incorporated phenol and are considered safer because the systemic absorption of phenol is naturally reduced. The chemical action produced depends not only on the phenol and the croton oil, but also on the number of layers, the exposure time, and the pressure put on applying the agents or even on how the skin is covered with the tape mask for occlusion.
Nevertheless, one of the significant obstacles in handling these products lies in how difficult it can be to obtain and reproduce the different formulae. In other words, it is difficult to know for sure what specific formulation is inside a small 3–4 ml vial and be absolutely confident in the use of it. One possible solution to this could be the creation of internationally approved, standardised guidelines. The existence of further regulation is important for the creation of approved formulae that can be reproduced and aid both the learning and the teaching of the technique.

