

The aesthetic industry in Asia
Over the past decade, Asian economies have grown exponentially, resulting in increased personal wealth and subsequent consumption of cosmetic procedures. Interestingly, though not surprisingly, cosmetic surgery procedures on Asian patients in Western countries have also seen a growth pattern parallel to Asia. As this growth continues, facial plastic surgeons in Western nations will inevitably see an increased number of Asians among their patient population. To meet this demand, the aesthetic doctor must incorporate a set of different aesthetic norms from the traditional Western philosophies in addition to understanding the unique cultural motivations for surgery. As previously mentioned, the Asian face has distinguishing features that are unique. As such, surgical techniques and aesthetic goals for a particular cosmetic procedure must be different to those for other ethnic groups. Tellingly, the three most common cosmetic procedures unique to the Asian face remain blepharoplasty, Asian rhinoplasty, and in recent years, jawline contouring.
The demand for lower facial contouring has increased exponentially over the years. This phenomenon seems to be limited mainly to Asian populations. One reason could be because the Asian view of beauty is different to that of Caucasians. They tend to equate femininity with beauty. Thus, a face that exudes a softer facial shape with delicate features is inherently preferred to squarer faces with stronger, more masculine attributes. This explains the surge in popularity in procedures that help one to achieve the V-shape face, which is said to be more feminine.
Treatment of the masseters
The overall Asian facial structure is typically classified as brachycephalic or mesocephalic, with a widened mandibular arch and resulting broad-looking lower facial skeleton.
Jawline contouring has been traditionally addressed with surgical excision of a prominent mandibular angle or convex mandibular body. This treatment is effective for permanent jawline contouring; however, it is associated with known complications and prolonged recovery time. An effective and alternative non-surgical treatment for a prominent jawline can be achieved using botulinum toxin. The toxin is used to selectively treat areas of the masseter muscle to promote atrophy of this muscle along the mandibular angle, resulting in a contoured jaw. While this was previously a treatment reserved for bruxism or teeth grinding, recent years have seen this treatment being administered for the sole aesthetic purpose of slimming the jaw.

Figure 2 Neurotoxin treatment of masseters can lead to a tapering of the lower facial shape.
Culturally, female Asian facial beauty is characterised by an oval facial structure. Contributing to this shape, the aesthetic lower face gently tapers medially from the ear lobule to the body of the mandible. While a wide mandibular arch is prevalent among Asians, there are inherent culturally negative attributes associated with a strong jawline — especially for females. To address this, a number of non-traditional therapies have been developed to specifically address a wide mandibular arch ranging from massage therapy to acupuncture. Anatomic structures contributing to this shape include a prominent mandibular angle, a convex mandibular body, parotid gland hyperplasia or tumour, excessive subcutaneous fat, hypertrophic masseter muscle, and a foreshortened chin.
Procedure
Prospective patients are evaluated for masseter bulk, mandibular ramus prominence, facial nerve symmetry, and jawline symmetry. Asymmetries are confirmed with the patient prior to treatment. Careful photography is taken at three positions, namely full frontal and at 45 degrees from the frontal position bilaterally. This is important to document any pre-existing asymmetries that may be present, as well as track improvements to the jawline after treatment.
Injection to the masseters is a comfortable procedure for most patients, especially when undertaken with a 33 G needle. Topical anaesthetic (e.g. EMLA) is not normally required, but can be offered to anxious patients if desired. If topical anaesthetic is required, it is usually applied 10 minutes before treatment.
The inferior insertion of the masseter muscle into the mandible is marked along the inferior border of the mandible. The patient is asked to ‘bite down’, occluding his/her teeth tightly, while the muscle bulk is palpated. Depending on the muscle bulk, two-to-three equidistant points are marked within the borders of the masseter muscle. In smaller ladies, it is sometimes usual to have only one or two points of injection. The muscle should be treated maximally
at the bulkiest point, with smaller doses placed at the periphery of the muscle. It is also prudent to remember that botulinum toxin injections have an area of diffusion, therefore, multiple injections may not always be necessary, especially in a patient with a smaller masseter.
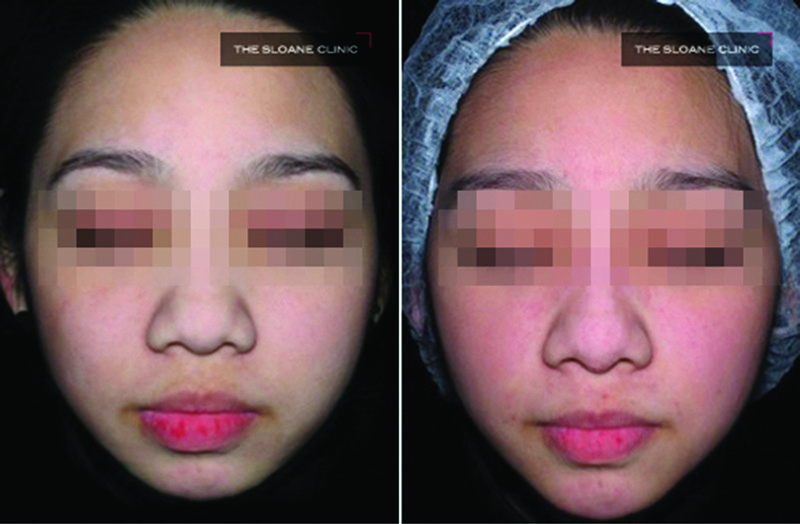
Figure 3 Augmentation of the chin with dermal fillers to improve mandibular contour and projection.
In general, a patient’s initial treatment requires injection of 24–32 units of onabotulinumtoxin A (Botox; Allergan, Irvine, CA) on each side. This amount is variable and will largely depend on the doctor’s assessment of the patient and the patient’s needs.
As treatment of the masseter is now largely done for aesthetic indications, the doctor will have to take into account the desired endpoint and the amount of slimming required to achieve it. The doctor should also consider the other facial features and proportions, which may affect the final result. For example, a patient with a very slim face who desires only slight slimming of the masseters may be treated with a lower dose of onabotulinumtoxin A as compared with another patient who has more severe masseter hypertrophy and a history of long-standing bruxism. Depending on any pre-existing asymmetries, the dose of onabotulinumtoxin A can be adjusted on each side to correct this.

