

Figure 4 Rectangle face
Group 1
Thirty patients with a triangular-shaped face (Figure 2), often presenting with slight wrinkles. The subcutaneous tissue is very thin and friable, and in many cases, there are signs of atrophy (even prior to menopause).
Group 2
Thirty patients presenting with a round-shaped face (Figure 3), and who most often have combined types of ageing with displacement of surface fat packages in the middle third of the face. Deep fat begins to display atrophic changes.
Group 3
Thirty patients with a rectangular-shaped face (Figure 4), and showing greater signs of ageing: subcutaneous adipose tissue hypertrophy and a migration of fat packages in the mid-face, resulting in the appearance of deep nasolabial folds. Hypertrophy of the subcutaneous fat on the edge of the mandibula and its displacement with the appearance of a square-shaped face. Hypertrophy of the subcutaneous fat in the area of chin results in the appearance of a double chin.
After dividing the patients into these groups, the authors then divided the patients from groups 1 and 2 into two further groups according to the principles of randomisation. Group 3 was not included owing to presentation with subcutaneous adipose tissue hypertrophy, what meant that in most cases this cohort required treatment with the bolus technique, and not the dot technique.Both before and after treatment, results of facial volumisation were compared with Ascher’s levels of ageing and facial tissue depression.
Half of the patients (n=30) were injected using a traditional volumising technique (i.e. bolus) with approximately 2 cc per side (4 cc per patient) of Juvéderm VOLUMA. It was found that Ascher levels 3–4 were reduced to levels 1–2 after only one procedure. The remaining 30 patients were injected according to the principles of the LIFT Concept, and reaped the same results (Ascher levels 3–4 to Ascher levels 1–2). In this arm of the study, the authors injected 1 cc per side to 80% of patients, and 1.5 cc per side to 20% of patients. The results were stable for 18–20 months in all patients.
All patients were also administered injections of botulinum toxin A (onabotulinumtoxin A). Before injecting, the patient’s face was analysed to assess muscular hyperactivity. All patients were informed that ‘on-label’ treatment targets only the glabella area (including forehead lines and Crow’s feet), but that treatments elsewhere on the face are ‘off-label’ in the majority of cases.
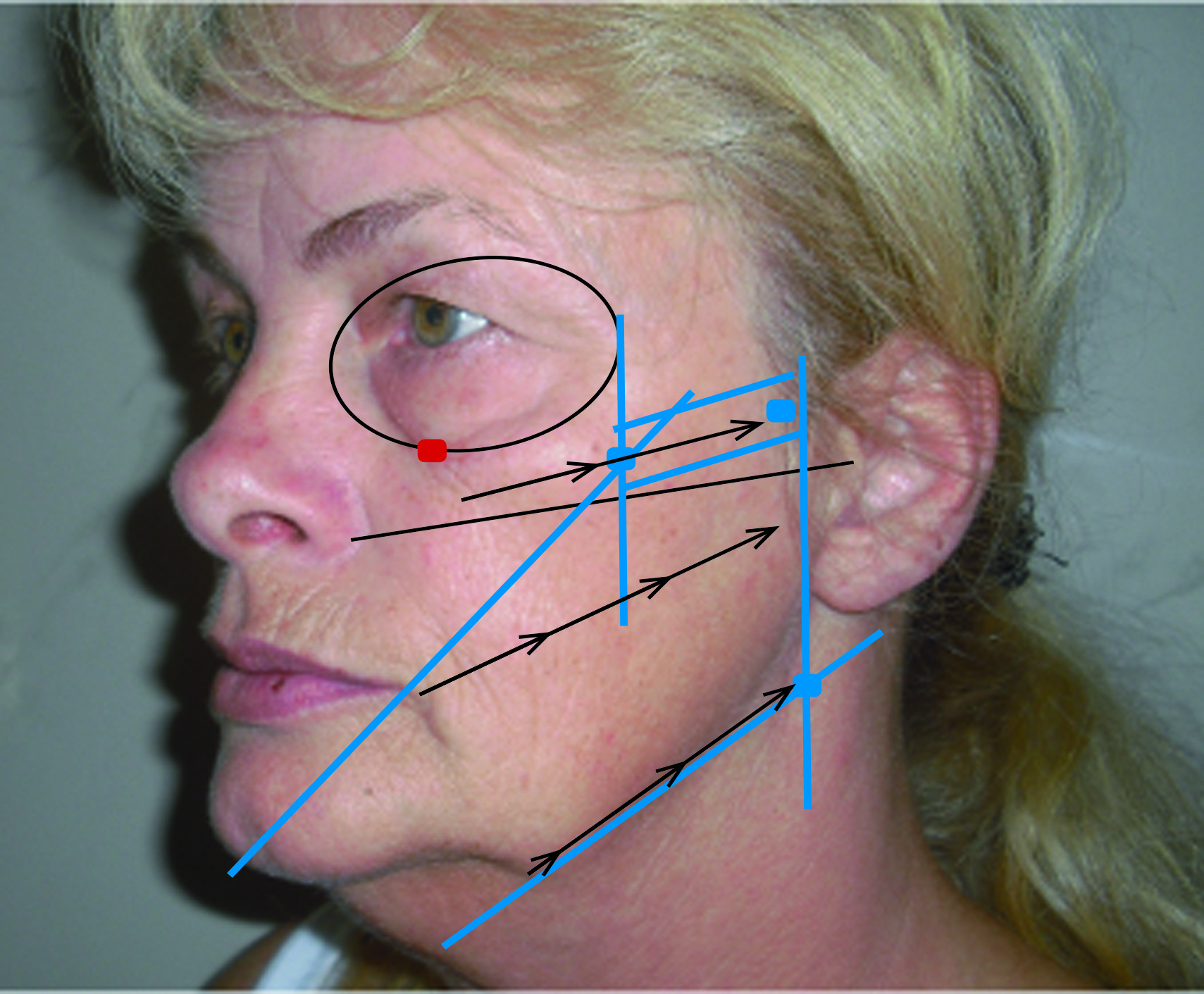
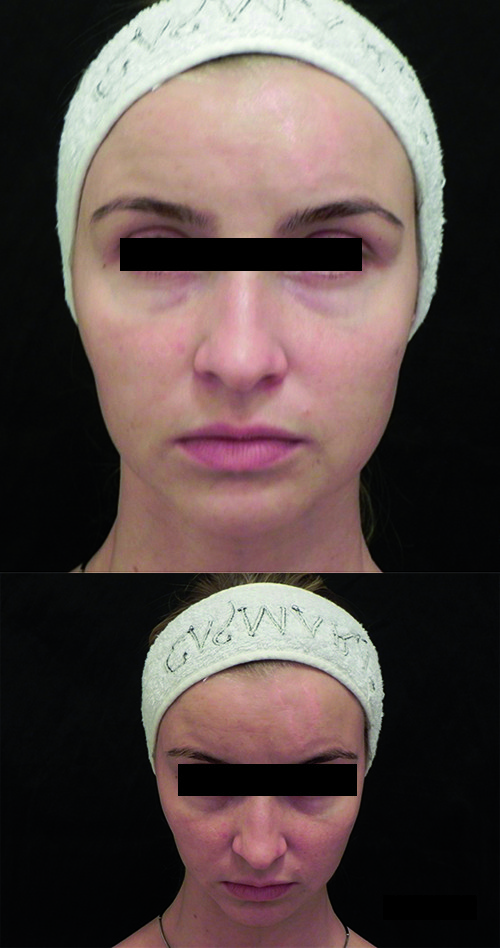
Figure 5 Triangular face (left) before and (right) after. 2.0 ml monophasic highly cohesive filler that consists of cross-linked hyaluronic with low-molecular-weight
Results
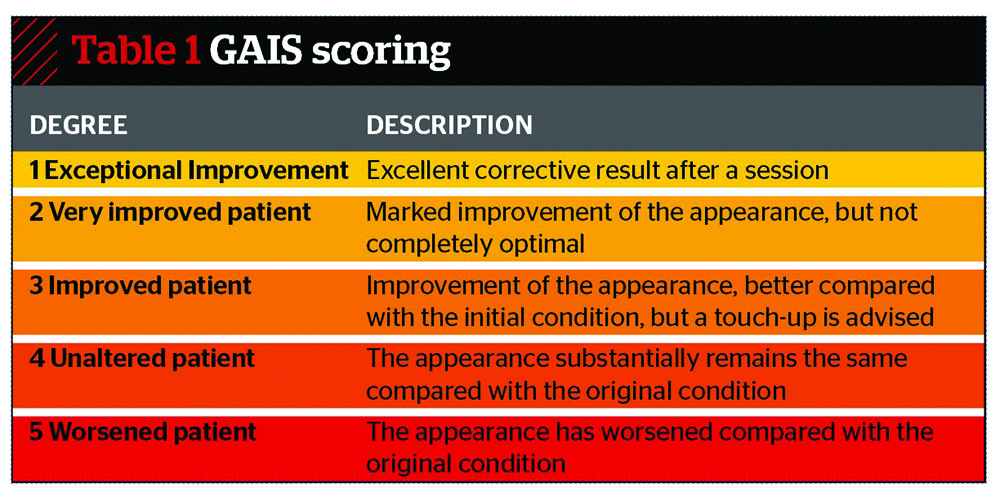
All patients were asked their opinions and the results analysed according to the Global Aesthetic Improvement Scale (GAIS). The results as analysed by the patients in group 1 were (see Table 1): 1=40%; 2=45%; 3=10%; 4=4%; 5=1%. Results in group 2 were: 1=50%; 2=43%; 3=3%; 4=4%; 1=0.
The authors attempted to analyse the areas in which thew hyaluronic acid was injected, the quantity and the results and the interesting conclusion appears; the quantity is much less important in comparison with the correct positioning. This idea is not new and has been described in the literature5, 6. However, in this study it is proposed that those right places are the dots of possible injection where the face bones are closest to the skin, where the soft tissues are thinnest, and therefore, where the smallest possible amount of filler can be used.
It is also paramount to position correctly at the temporal area and on the mandibular. Furthermore, once the correct place has been found, it is necessary to inject very carefully and not to inject more than needed. The best solution is to use a monophasic highly cohesive filler consisting of cross-linked hyaluronic acid, and with a high proportion of low-molecular-weight short chains with an optimum viscosity and cohesion.

Figure 6 (left) Before and (right) after. 0.6 ml monophasic highly cohesive hyaluronic acid filler
The technique proposed by the authors is useful for a number of reasons. The ‘dot’ technique is very safe for the patient, with no risk of ischaemia or hyper-volumisation. The technique can be used by any professional with a good knowledge of anatomy and understanding that it is more useful for those patients with thinner and less sub-skin fat, who have experienced only mild volume loss and fat migration.
Conclusions
It is necessary to start volumisation in ageing patients carefully, taking into account the type of face and to combine treatment with botulinum toxin. If hyaluronic acid is injected at the precise ‘dots’ using all the principles described in this article, it is possible to achieve a successful result using approximately 2-times less product, combined with botulinum toxin.
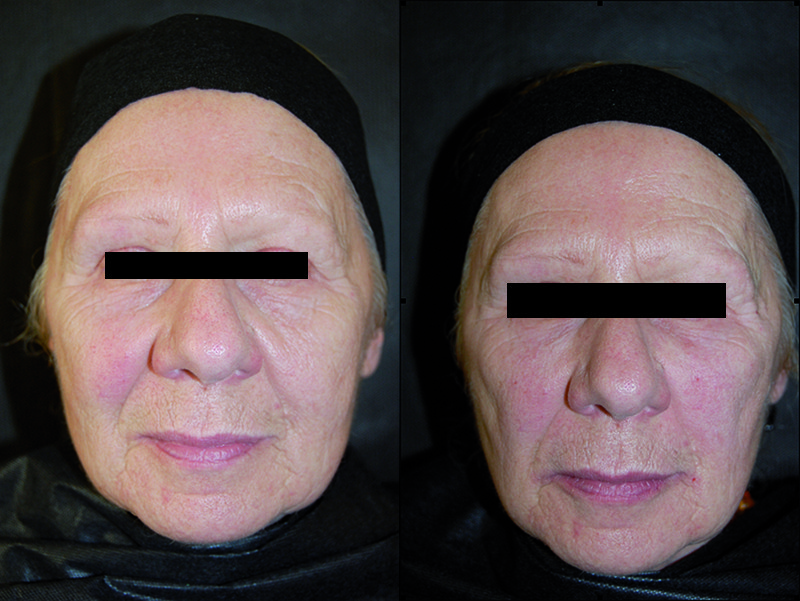
Figure 7 Round face before (left) and after (right). 2.0 ml monophasic cross-linked hyaluronic acid with a high proportion of low-molecular-weight short chains, plus 1.0 ml standard hyaluronic acid
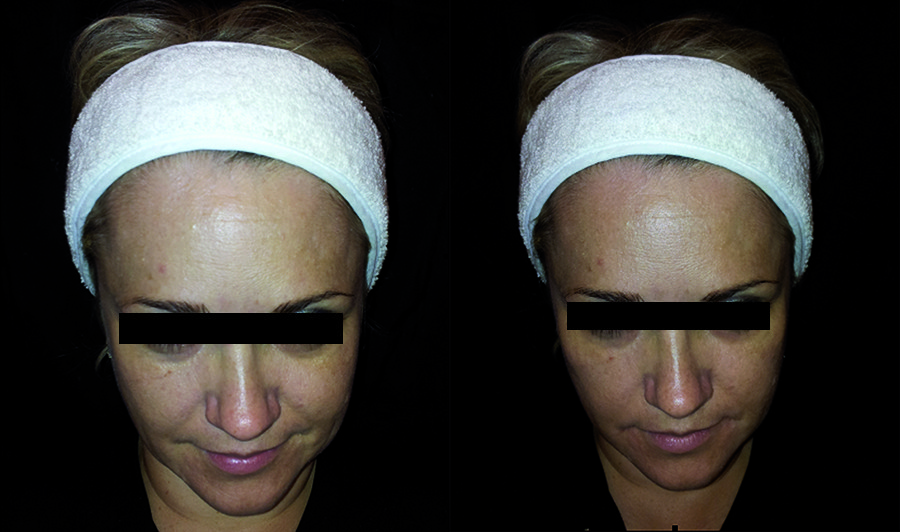
Figure 8 Before (left) and after (right). 1.0 ml monophasic highly cohesive filler consisting of cross-linked hyaluronic acid with a high proportion of low-molecular-weight short chains

