

Case report
Past medical mistory

Figure 3 Treatment to the crow’s feet with botulinum toxin A, (A) before treatment and (B, C, D) 3 weeks after treatment. Twelve injection points to the orbicularis oculi. Each side received three injections of 2 U intramuscularly (green) and nine injections of 0.5 U intradermally (purple). (Total dose 11 U per side)
The 45-year-old female patient presented in 2009 with a profound volume loss in her mid-face, but also in the perioral region, as well as early hyperkinetic wrinkles and mimetic folds. Until she presented at the clinic, she had never received any aesthetic procedure, apart from regular medical facials as a result of acne vulgaris, and consistently used sun protection. The patient was healthy, with no allergies, no history of operations, no infections, and was not taking any medication.
Evaluation and diagnosis
The area of concern was the patient’s face, focusing on expression lines and a loss of volume in her mid-face.
At rest, the glabellar and forehead lines marked 2 on the Merz Scale (MS)10 (moderate lines), and with a mark of 4 at maximum contraction (very severe lines). The crow’s feet were MS 3 at rest (severe wrinkles) and MS 4 (very severe wrinkles) at maximum contraction
Infraorbital hollowness was MS 4 (very severe hollows), with upper and lower dermatochalasis and protrusion of lower eyelid fat pad. The nasiolabial folds were marked at MS 4 (very severe fold), the upper mid-face at MS 3 (severely sunken upper cheek), lower mid-face at MS 4 (very severely sunken lower cheek), oral commissures at MS 4 (very severe downturn), upper-lip rhytides at MS 2 (moderate wrinkles), upper and lower lip volume at MS 3 (thick), and the jawline at MS 3 (severe sagging).
There was also prominent volume loss to the mid-face (MS 3–4) and a loss of contour to the jawline (MS 3), as well as static wrinkles (MS 2–4) and severe mimetic wrinkles (MS 2–4). The patient also had signs of actinic elastosis.

Figure 4 Treatment to the nasolabial folds with dermal filler, (A) before treatment and (B) directly after treatment. This demonstrates the direct filling technique; linear threading with a short, sharp 27G needle, injecting Radiesse®, 0.5 cc per side, premixed with Lidocaine 1%
Therapy
In this article the author showcases the aesthetic treatments that this patient received over the past 7 years, from 2005 to date.
BoNT A
Treatment to the patient with BoNT A is shown in Figures 1–3. Approximately every 6 months, the mimetic wrinkles of the upper third of the face (glabellar lines, forehead lines, crow’s feet) were treated with BoNT A using Incobotulinumtoxin A, reconstituted in 1.25 cc, sterile, 0.9% unpreserved saline, using a 30 G needle.
Treatment was customised to the patient:
- ■ Glabellar lines received five injection points. 4 U intramuscularly to the procerus, 4 U per point medially, and 2 U per point laterally to the corrugator supercilii and depressor supercilii
- ■ The forehead lines had 12 injection points. The frontalis muscle was injected intramuscularly — six points at 2 U (medial, lateral cranial) and six points at 1 U intramuscularly and medially (including two points to the lateral eyebrow), and intradermally and laterally
- ■ The crow’s feet had 12 injection points. The orbicularis oculi had three injections intramuscularly, each at 2 U; nine injection points were intradermal, each at 0.5 U
- ■ Overall doses: glabellar lines 2 U, forehead lines 10–20 U, and crow’s feet 6–10 U per side.
Dermal filler
To the nasolabial folds (Figure 4), the author used a direct filling approach with linear threading, using a short, sharp 27 G needle. The product used was Radiesse® premixed with Lidocaine 1% in a 20% ratio. Total dose: 2 cc (1 cc per side).
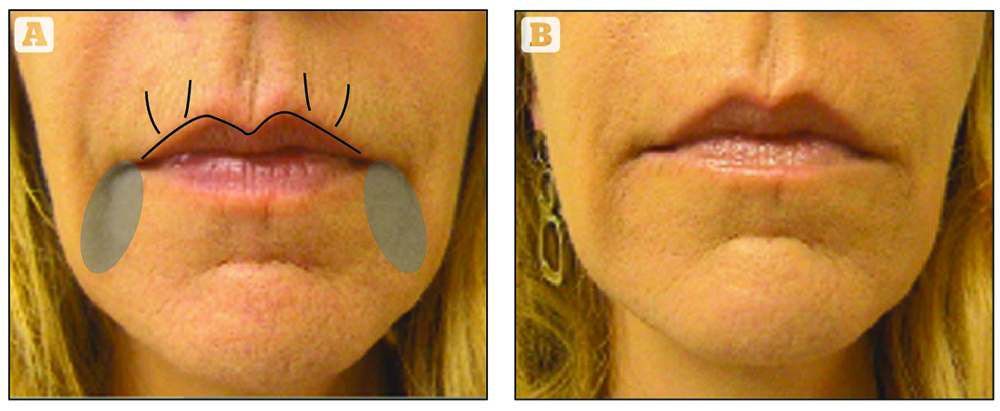
Figure 5 Treatment to the perioral region with dermal filler, (A) before treatment and (B) directly after treatment. Indirect filling technique to the upper lip; linear threading, 27 G blunt, 1.5-inch cannula, automated injection of Belotero Intense® 1 cc, premixed with Lidocaine 1%. Direct filling technique to the upper lip rhytides; linear threading with a sharp, short 30 G needle, Belotero soft® 0.5 cc. Corners of the mouth; linear threading and crosshatch, sharp, short 27 G needle, Belotero Intense® 1 cc
Treatment of the perioral region was three-fold (Figure 5). To treat upper-lip contours, an indirect filling approach was implemented with linear threading, using a 27 G blunt-tip, flexible, 1.5-inch cannula and an automated injection system. The total dose was 1 cc of Belotero Intense® premixed with Lidocaine 1% in a 20% ratio. For upper-lip rhytides, a direct filling approach was used with linear threading, using short, sharp 30 G needle. A total dose of 0.5 cc Belotero Soft® was administered. For the corners of the mouth, the author used the direct filling technique with linear threading and crosshatch, using a short, sharp 27 G needle. A total dose of 1 cc of Belotero Intense® was administered here.
In the periorbital region, the tear trough and lateral eyebrow were treated (Figure 6). The tear trough was treated using the direct filling approach with linear threading, using a short, sharp 30 G needle. A total dose of 0.6 cc Belotero Intense® premixed with Lidocaine 1% in a 30% ratio was used. The lateral eyebrow was also treated using the direct filling approach with linear threading, using a short, sharp 27 G needle. A total dose of 0.4 cc Esthélis Basic was administered.
The cheeks (Figure 7) were treated with an indirect filling and 3D vectoring technique with linear threading, using a 27 G blunt-tip, flexible, 1.5-inch cannula. A total dose of 1 cc (0.5 cc per side) of Radiesse® premixed with Lidocaine 1% in a 20% ratio was administered. Here, the author also used a direct filling and 3D vectoring technique with a bolus 27 G, short, sharp needle to administer 1.5 cc of ReDexis® Ultra.

Figure 6 Treatment to the cheeks with dermal fillers. (A) Before treatment and (B) directly after treatment, using an indirect technique of 3D vectoring; linear threading with a 27 G blunt, 1.5 inch cannula,Radiesse® 0.5 cc per side, premixed with Lidocaine 1%. (C) After treatment, using a direct technique of 3D vectoring with a bolus 27 G, sharp, short needle, Redexis Ultra® 1.5 cc
Discussion
Today’s non-invasive treatments for facial rejuvenation by dermal filler and BoNT A injections are a lot more than just filling and relaxing wrinkles. Customised relaxation of hyperactive mimic muscles and a three-dimensional multiplane volumetry strategy enable the physician to lift and smooth facial structures individually and in an aesthetically appealing way.

Figure 7 Before (2005) (A) and after (2012) (B) total treatment
The doctor’s armamentarium for non-invasive aesthetic enhancement by injections should include a profound knowledge of anatomy and the product features of the injected dermal fillers and BoNT A. One should acknowledge study results on BoNT A and dermal fillers, and be able to break this knowledge down for the individual needs and aesthetic demands of their patients. Only advancements to our injection techniques and skills will lead to a refined aesthetic results in our patients.
Conclusions
The customised, individually adapted, conservative and intentionally low-dose treatment with BoNT A, as well as advanced dermal filler injection techniques with biodegradable dermal filler materials such as monophasic hyaluronic acid and calcium hydroxylapatite, enables us to globally reshape 3D facial structures in a safe, aesthetically appealing and natural way.

