Ekaterina Gutop looks at the options available and the points to consider when treating the upper face with botulinum toxin and fillers
Much has changed in the field of aesthetic dermatology. The industry has moved from a 2D to a 3D approach and the desire for a ‘dramatic’ result has evolved into the search for a ‘natural’ look; with more patients desiring a fuller face with a fresh and natural appearance after treatment. At the same time, new areas for correction, new products and devices for treatment, a deepening knowledge of the anatomy, and an understanding of the risks involved in each treated area as well as the required correction techniques affords practitioners a choice in respect to treatment protocols.
 Specific patient treatment requests should also be taken into account1. Frequently, a treatment plan is dependent on certain patient limits, such as time, budget, and fears. The author often categorizes patients into one of three groups: minimum, for patients seeking just one treatment; optimum, those requiring multiple injections to tackle a number of issues; and maximum, those with no limit on time and budget. The author believes this allows for the selection of the most appropriate individual treatment plan.
Specific patient treatment requests should also be taken into account1. Frequently, a treatment plan is dependent on certain patient limits, such as time, budget, and fears. The author often categorizes patients into one of three groups: minimum, for patients seeking just one treatment; optimum, those requiring multiple injections to tackle a number of issues; and maximum, those with no limit on time and budget. The author believes this allows for the selection of the most appropriate individual treatment plan.
The author is also able to categorize patients by focusing on the upper, middle, and lower thirds of the face dependent on treatment requests.
Patients who focus on the upper face request treatment for the areas around the eyes, such as glabellar lines, wrinkles on the forehead, deficiency of volume in the forehead and temple areas, palpebromalar groove, mid-cheek groove, and midface volume deficiency, which can lead to changes to the contour of the periorbital area relative to the tear trough.
Patients who request treatments for the lower third of the face, do so around the ‘classical zones’, such as nasolabial folds, marionette lines, and lips.
On the other hand, the mid-face is a key treatment zone for the majority of patients — in the upper, mid and lower portions of the face. By treating the mid-face with fillers, it is possible to achieve an improvement not only in the mid-face but in the lower and upper face too, including the tear trough and temple areas, nasolabial folds, and lower jowl contours.
The main aim of treatment is to improve the negative aspects of the face, transforming them to a positive, fresh-looking appearance, as well as beautifying and harmonizing the face without focusing on one zone for correction.
When planning the treatment protocol it is necessary to include an aesthetic analysis of the face, how the ageing process is affecting the various facial zones, and, after this, select the area, products, and devices for correction.
Each face is unique
Aesthetic analysis of the face
Analysis of the face should be the first stage of any aesthetic treatment. There are many characteristics that determine the harmonious face; the most important of them being the shape of the face, proportions, facial symmetry, volume harmony, and contours of the face. These characteristics should be analyzed in three projections: frontal, oblique and profile views1,3.
Key problem zones in these projections may be different and can be defined as zones that create a negative perception of the face. Expressions of anger, sadness, depression, and tiredness can be identified by a frown and lowering of the lateral parts of the brows, dark circles around the eyes, and drooping corners of the mouth1. At the same time, aesthetic markers of ageing may also give rise to negative characteristics in the face. Glabellar lines, crow’s feet, forehead lines, tear trough deformities, bags under the eyes, hollowing of the temples and cheeks, nasolabial folds, marionette lines, and jowls can all create a negative appearance. As a consequence, these ‘key’ negative characteristics should not be treated in isolation, but as part of a general treatment plan.
 Not only do the negative aspects of the face need to be analyzed but features that can be utilized to make the face more beautiful and harmonious should also be taken into account. For example, for women these ‘WOW’ zones can be areas that underline female gender characteristics of the face in general — lifting the lateral part of the brows, high cheekbones with the apex on their lateral upper-part, and sensual lips. Emphasizing these features via treatment can create a more attractive facial appearance. In addition, the facial analysis of mimic activity with different emotions before treatment helps to aid the performance of correction giving a natural result after treatment not only in static but also in dynamic lines.
Not only do the negative aspects of the face need to be analyzed but features that can be utilized to make the face more beautiful and harmonious should also be taken into account. For example, for women these ‘WOW’ zones can be areas that underline female gender characteristics of the face in general — lifting the lateral part of the brows, high cheekbones with the apex on their lateral upper-part, and sensual lips. Emphasizing these features via treatment can create a more attractive facial appearance. In addition, the facial analysis of mimic activity with different emotions before treatment helps to aid the performance of correction giving a natural result after treatment not only in static but also in dynamic lines.
When planning individual treatment protocols for correction it is vital to take into consideration the differentiation between individual aesthetic peculiarities and the ageing processes of the face.
No two faces are alike
Anatomical analysis of the face
Every face is multi-layered and individual by nature2, 5, 7. The face of the patient in general and problem zones in particular have to be analyzed from an anatomical point of view.
First, the appearance of the face is dependent on the color and quality of the skin. The color and it’s evenness, texture, elasticity, and signs of ageing, such as wrinkles and folds have to be taken into account and may be corrected in a variety of ways. Different options such as chemical peels, cosmeceuticals, energy-based devices, and injections of hyaluronic acid and meso-cocktails may be used to improve the color and quality of the skin.
The first signs of ageing skin may be found in the periorbital area and influence the appearance of this area in particular and look of the face in general.
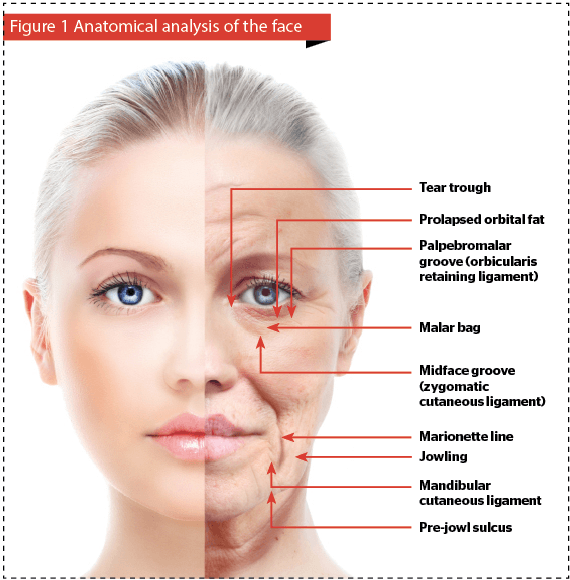
 Deep and superficial fat compartments have different thicknesses in different areas of the face7, 10. In the upper face, superficial fat compartments, such as the central and middle forehead, lateral temporal-cheek compartment, lateral orbital, and medial fat compartments are individual by nature and separated by fibrotic bands, which connect the dermis to the SMAS2,10,6. The weakening of ligaments, such as the zygomatic or orbital retaining ligament, and the protrusion of fat compartments above them cause the age related changes of the facial contours, including bags under the eyes, nasojugal groove, palpebromalar groove, and malar bags6, 10. Deficiency of volume in the upper and mid face, caused by hypotrophy of the deep malar fat compartment, has to be identified as a target zone for correction with fillers4, 6.
Deep and superficial fat compartments have different thicknesses in different areas of the face7, 10. In the upper face, superficial fat compartments, such as the central and middle forehead, lateral temporal-cheek compartment, lateral orbital, and medial fat compartments are individual by nature and separated by fibrotic bands, which connect the dermis to the SMAS2,10,6. The weakening of ligaments, such as the zygomatic or orbital retaining ligament, and the protrusion of fat compartments above them cause the age related changes of the facial contours, including bags under the eyes, nasojugal groove, palpebromalar groove, and malar bags6, 10. Deficiency of volume in the upper and mid face, caused by hypotrophy of the deep malar fat compartment, has to be identified as a target zone for correction with fillers4, 6.
The individual characteristics of mimic muscles (procerus muscle, corrugator supercilii muscles, orbicularis oculi muscles and frontalis muscle) with their volume, activity and muscle asymmetry have to be analyzed as a target area for correction with botulinum toxin injections (BoNT-A)2,7,10,12.
Bone structures (orbital rims, cheek bones, bones of the temporal area) with individual anatomical peculiarities, such as hypoplasia, bone asymmetry, or age related changes should be observed and palpated because they are not only anatomical markers but also a target zone for treatment with volumizers (Figure 1)2,10.
Treatment plan
When formulating the treatment plan, aesthetic and anatomical peculiarities of the patient, and the individual nature of the ageing processes have to be taken into account1. The key problem zones of the face are very individual by nature but the most commonly encountered in the upper face are horizontal and glabellar lines, lowered eyebrows, crow’s feet lines, changes of volume in the temporal and forehead areas, and age related changes at the periorbital area. The most commonly performed treatments for the upper face are injections of botulinum toxin and hyaluronic acid fillers (HA fillers), according to the specific indications. The choice in area for correction, choosing the appropriate products considering volumes and doses, and suitable correction technique are at the preference of the doctor.
When a patient presents with not one but several areas that need correction, the treatment should begin with the most evident zone and continued step by step along the others. In such cases, treatment can be performed over several sessions.
Upper face treatment with BoNT-A
Treatment with BoNT-A can be a separate procedure or also one part of the integral treatment of the face. Individual requests from the patient for a fresh look, opened eyes, lifted brows, and maintenance of mimic activity with the absence of wrinkles dictates the individual approach in concentration, points, and doses of botulinum therapy11.
 Additionally, the use of the standard in BonT-A treatment of 20 units in the glabellar area affords us the possibility of achieving not only the elimination of wrinkles but also targeted blocking of mimic activity for the whole period of the product’s action12. The indications for aesthetic treatment with botulinum toxin vary in different countries, but the most commonly approved indications are glabellar lines, crow’s feet, and forehead lines.
Additionally, the use of the standard in BonT-A treatment of 20 units in the glabellar area affords us the possibility of achieving not only the elimination of wrinkles but also targeted blocking of mimic activity for the whole period of the product’s action12. The indications for aesthetic treatment with botulinum toxin vary in different countries, but the most commonly approved indications are glabellar lines, crow’s feet, and forehead lines.
Treatment with BoNT-A has been described in a large quantity of publications and therefore will not be discussed in details in this article12. Combined treatments protocols with BoNT-A and, simultaneously, with fillers for the upper face are frequently requested by patients and accomplished by the doctor.
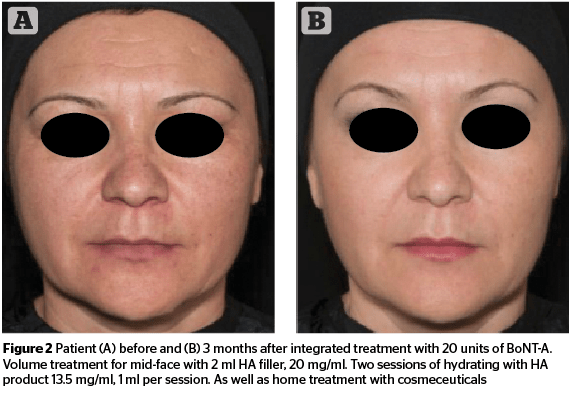
Planning the treatment with BoNT-A and fillers in one session, it is preferable to start with filler injections and finish with botulinum toxin. The main reason for this is the necessity to model the filler in the treated area after injection, especially in the lateral or medial part of infraorbital area as well as the medial part of the temporal area.
When planning treatment with injections of botulinum toxin and fillers over two sessions, injections of BoNT-A should be made first and treatment should be continued 2–4 weeks after with filler injections
(Figure 2).
Upper face treatment
with fillers
Periorbital area and mid-face
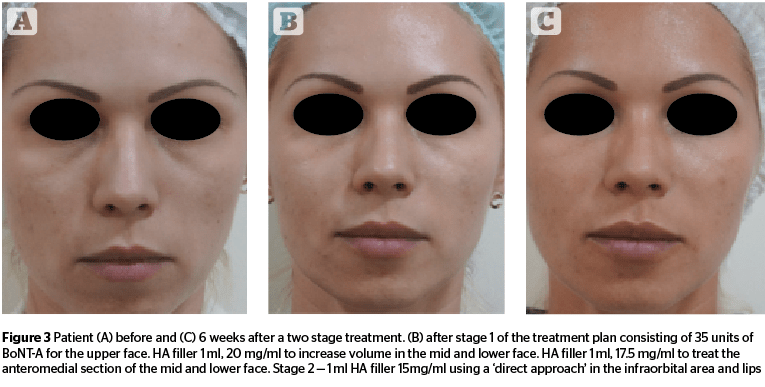
The treatment of the periorbital area can be completed using two methods. The ‘direct approach’ in treatment is more suitable for patients with a nasojugal groove when volume of the anterior part of the mid-face is still adequate. In the author’s opinion, the safest way to perform this treatment is using a cannula with a HA filler (0.2 ml) in a retrograde or microbolus technique. Slight under-correction by 10–15% immediately after treatment is acceptable and highly recommended.
The choice of cannula is governed not only by the wish to minimize side-effects in the form of bruising and swelling, but also by the diagnostic possibility to identify accurately when passing through the zygomatic ligament, orbital retaining ligament, and orbital muscle due to the resistance to the cannula2,5. A hyaluronic acid product with the minimum hydrophilic profile should be injected in the infraorbital area (Figure 3).
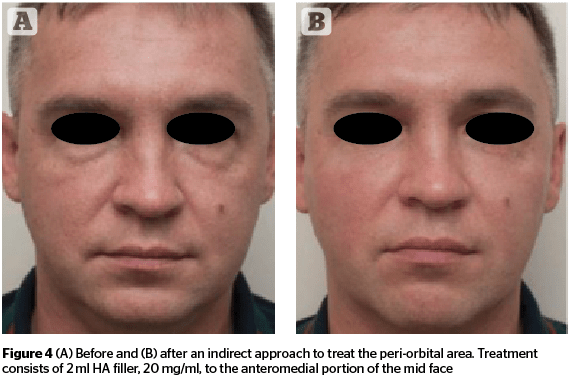
An ‘indirect approach’ should be used in the periorbital area to treat volume deficiency in the anteromedial area of the mid-face.
 Volume treatment in this area helps to achieve an improvement not only in volume loss in the mid-face but also to mask problems in the infraorbital area. HA products with high G’ are more suitable when volume loss is due to a deficiency in the bone structure (Figure 4)9. When volume deficiency is associated with age related changes in volume loss in the deep malar fat compartment, products with a medium viscosity and lifting capacity are preferred.
Volume treatment in this area helps to achieve an improvement not only in volume loss in the mid-face but also to mask problems in the infraorbital area. HA products with high G’ are more suitable when volume loss is due to a deficiency in the bone structure (Figure 4)9. When volume deficiency is associated with age related changes in volume loss in the deep malar fat compartment, products with a medium viscosity and lifting capacity are preferred.
Whether to use a needle or cannula for the indirect approach is at the preference of the doctor. Using needles helps to minimize the quantity of product in the appropriate area. Performing an aspiration test; determining the level of insertion of the needle into the superficial fat compartment; and avoiding damage to or compression of the infraorbital artery, vein, and nerves when performing the procedure are vital and help to complete the treatment in the most effective way. On the other hand, using a cannula in this area helps to complete the procedure in a safer manner than compared to needles.
Temporal area
The author has never experienced a patient request to solely treat the temporal area. Therefore, this area should be pointed out to the patients and, as it is usually one stage of the complete facial treatment, the importance of the treatment should be explained. The correction technique is dependent on the goal of the treatment. The most common indications for treatment with fillers in this area are to smooth the transition from the cheekbone area after correction of the lateral part of the cheekbone or to directly treat age related lipoatrophy and volume loss in the temporal area directly.
In both cases, treatment in the temporal area should be based on the indications, anatomical peculiarities of the face, and knowledge of anatomy including vascular structures (i.e. sentinel vein, superficial temporal artery, and temporal nerve).
Deep temporal injections are suitable for the correction of volume loss8. Injections should be performed with a needle. To minimise the risk of vascular complications, use a HA product (0.5–1.0 ml) with a high G’ via the bolus technique in each temple, remembering to aspirate when touching bone and inject only after a bubble has appeared in the syringe.
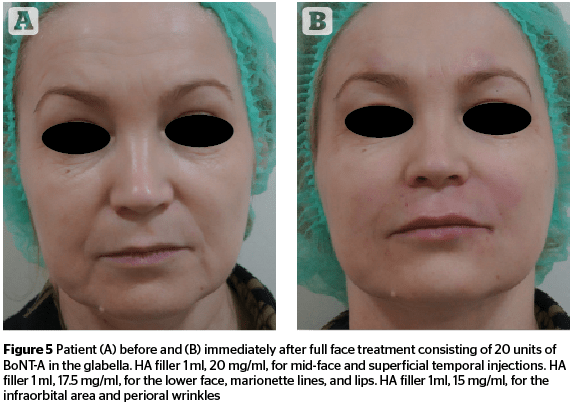
A superficial temporal injection can be performed to smooth the transition from the temples to the lateral area of the cheekbone. It is vital to use a 25G cannula with a line fanning technique below the superficial fascia using HA product with high characteristics of plasticity and the appropriate volume of the product (not more than 0.2 ml because of the limited space in this area) (Figure 5).
The disadvantage of superficial temporal injections is the high risk of damaging vessels. Also, there is a high risk for protrusion of superficial veins when an excess amount of product is injected.
Lower brow lift
Lifting of the lateral eyebrow is one of the most frequently requested treatments among patients for which botulinum toxin injection is generally recommended. These can be supplemented by the use of fillers.
Basically, the goals of the treatment with fillers in this area are lifting the eyebrows, correction of volume loss, and, creating the contrast of light and shadow. A bolus injected with needle or cannula with the appropriate volume of no more than 0.2 ml of should be used.
It is vital to take into account the relationships between the position of the eyebrows and orbital rim. When eyebrows are located below the upper orbital rim treatment with fillers in this area can cause the opposite intended result, such as heaviness of the lateral part of the brows.
Circumvention of complications
The key rules to follow to ensure a safe treatment include, respect for anatomy, using the small bolus technique, slow injections, aspiration, using cannulas, and choosing the appropriate volume and correction technique for the appropriate layer in the appropriate areas.
Because of the variety in anatomy there is no full guarantee of safety for injections in the upper face; therefore dynamic observation of the patient after procedure, timely diagnosis, and immediate treatment in case of complications are vital for success.
Conclusion
Planning a full face treatment, the practitioner must take into account the main goal of treatment is to emphasize the individual beauty of the face.
It is often said that ‘the eyes are the mirror of the soul’; therefore, the appropriate treatment protocols for the areas around the eyes should achieve an improvement for the face in general. Harmonization of the face, based on individual aesthetic and anatomical peculiarities, and a logical approach to the sequence of stages in treatment protocols, helps to obtain a natural result in the most convenient way for both the doctor and the patient.