

Botulinum toxin A
Botulinum toxin A immobilises local muscles, reduces skin tension caused by muscle pull, and thus, decreases microtrauma and subsequent inflammation65. Reduction of the tensile force during the course of cicatrisation and effective regulation of the balance between fibroblast proliferation and cellular apoptosis66 may represent a novel therapeutic option for the aesthetic improvement of post-surgical scars. Gassner et al studied 31 patients undergoing elective excisions of cutaneous neoplasms of the forehead in a prospective, blinded, placebo-controlled study67. Patients were randomised to botulinum toxin (0.2 ml of preservative-free normal saline with 15 U of botulinum toxin A (Botox, Allergan, Irvine, California) per 2 cm intraoperative length) versus placebo (0.2 ml of preservative-free normal saline) injection into the musculature adjacent to the wound within 24 hours of wound closure. At 6-month follow-up, the overall median visual analogue scale score for the botulinum toxin-treated group was 8.9 compared with 7.2 for the placebo group, indicating enhanced healing and improved cosmesis of the experimentally immobilised scars67. By injecting botulinum toxin 4–7 days prior to surgery, the authors have seen similarly convincing results using a comparable dosing regimen, depending on the respective anatomic location.
Intralesional injection of botulinum toxin has also been proposed for the treatment of established keloids in a prospective, uncontrolled study68. Botulinum toxin A was injected into the lesions at 3-month intervals for a maximum of 9 months at a concentration of 35 units/ml. Total doses ranged from 70 to 140 units per session. At 1-year follow-up, three of the 12 patients demonstrated excellent, five good, and four fair results. The therapy did not fail in any of the patients. When analysing clinical symptoms, scar regression was noted from the periphery in all of the patients followed by flattening of the lesions. Within the follow-up period of 1 year, no signs of recurrence were noted in any of the patients. As a mechanism, the same group could then demonstrate that botulinum toxin is able to reduce the expression of TGF-β1 protein in fibroblasts derived from scars and significantly reduce their proliferating rate69.
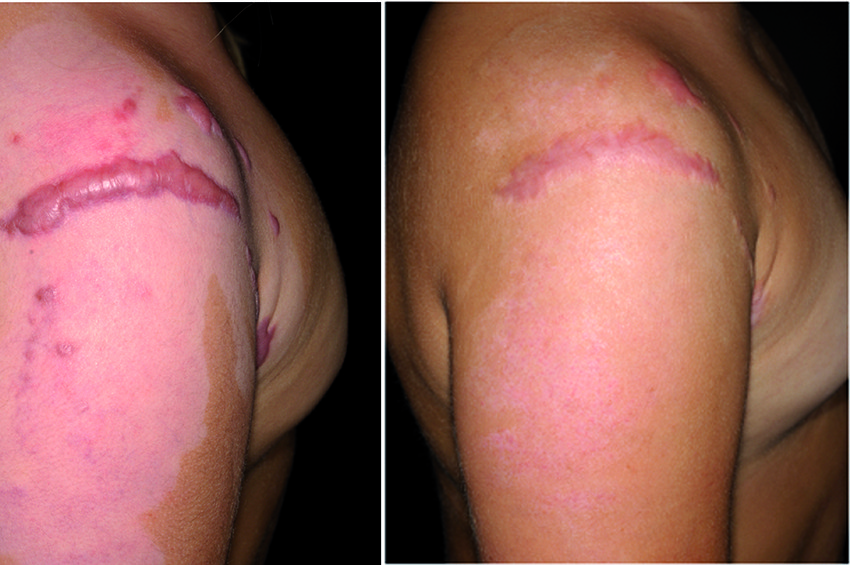
Figure 4 Pressure garments represent a promising means in treating excessive scarring, demonstrating convincing results (particularly in children). (left) before treatment and (right) result after 4 months (12 hours per day)
However, in a recently published study, objective evaluation of botulinum toxin-treated keloids using optical profilometry did not reveal any changes after therapy compared with baseline70. Consequently, while reduction of the tensile force by prophylactic botulinum toxin A injections into the musculature adjacent to the respective wound during the course of wound healing and scar formation might represent a comprehensible mechanism of action for the aesthetic improvement of post-surgical scars, the suggested clinical efficiency of intralesional botulinum toxin for the treatment of existent keloids remains uncertain. Certainly, more in-depth studies on the effects of the toxin on pathologic scars and/or mature keloids are needed before a comparatively expensive therapy for this particular indication can be postulated.
Current and emerging approaches for keloid and hypertrophic scars
An increasing number of patients are disappointed with their scars, as demonstrated in one American survey71. Many patients would value any opportunity to improve or minimise scarring following surgery or trauma71 and seek medical help for the improvement of appearance of existing unpleasant scars. Based on the German Guidelines for the treatment of pathological scarring, most of the propagated therapeutic approaches may be used for both hypertrophic and keloid scarring23. Nevertheless, clinical differentiation between hypertrophic and keloid scars (according to Mancini2 and Peacock3) is paramount before the initiation of any treatment — particularly before starting any surgical or ablative laser-related manipulations, owing to increased recurrence rates with keloids.
Intralesional corticosteroid injections
Intralesional steroid injections have gained popularity as one of the most common approaches to improve hypertrophic scar and keloid formation since the mid-1960s72. Effects of corticosteroids primarily result from their suppressive effects on the inflammatory process in the wound36, and secondarily, from reduced collagen and glycosaminoglycan synthesis, as well as inhibition of fibroblast growth73. Three to four injections of triamcinolone acetonide (TAC; 10–40 mg/ml) every 2–4 weeks are generally sufficient, although injections continue for 6 months or more72. When used alone, intralesional corticosteroid injections have the best effect on younger keloids and can provide symptomatic relief.
For older hypertrophic scars and keloids, combination with cryotherapy may show more effective results74, 75 and represents the most widely used modality in the authors’ daily practice. Indeed, the combination of cryotherapy with intralesional TAC injections seems to yield marked improvement of hypertrophic scars and keloids76–78. The authors recommend cryotherapy directly before the administration of intralesional TAC injections, as success rates appear to be increased based on the larger amount of TAC that can be injected owing to dermal oedema formation caused by cryotherapy. Side-effects include dermal atrophy, telangiectasia (Figure 5), and pain at the site of injection. The latter can be avoided by using a topical anaesthesia and/or regional injections of local anaesthetic around the scars to be injected79.

