

Hair microPigmentation Treatment (HPT®), more commonly known as scalp micropigmentation or scalp tattooing, is a revolutionary semi-permanent micro-pigmenting technique that offers an alternative option for both men and women experiencing hair loss who are not appropriate candidates for hair restoration surgery or who do not want it. HPT involves the use of a digitally controlled needle to apply medical grade hypoallergenic colour pigment into the scalp to create the illusion of ‘hair’ follicles. Scalp micropigmentation to date has most widely been used as a solution for male pattern baldness. In the majority of cases the procedure is used to give the patient the illusion of a closely shaven head or cropped appearance. However, as a complimentary hair loss solution HPT can effectively be used to camouflage transplant scarring from older type hair restoration surgeries or enhance successful hair restoration procedures. Additionally, the treatment can be used to camouflage diffuse thinning and female pattern hair loss, where alternative options are more limited for female patients.
Hair loss, or alopecia, in its variety of forms, affects millions of people worldwide. Indeed, according to a recent study undertaken by Relevant Research Inc., on behalf of the International Society of Hair Restoration Surgery (ISHRS), 35 million men and 21 million women in the US alone suffer from this condition1. Androgenetic alopecia (AA), more commonly known as male or female pattern baldness, is by far the most common form of hair loss.
Hair loss
Male pattern baldness accounts for more than 95% of hair loss in men. By the age of 35 almost two-thirds of men will experience some degree of appreciable hair loss, rising to 85% by the age of 50. While there are many reasons why men lose their hair, the majority of male pattern (AA) baldness cases are heredity and the sufferer has inherited a genetic sensitivity to dihydrotestosterone (DHT). Male pattern baldness is generally characterised with the onset of a receding hairline and thinning crown, as these areas appear to be the most sensitive to DHT. This pattern eventually progresses into more apparent baldness throughout the entire top of the scalp, often leaving only a rim or ‘horseshoe’ pattern of hair in the more advanced stages of male pattern baldness.
Hair loss in women falls into two distinct categories — female pattern hair loss, which accounts for about 95% of cases, and chronic hair loss. The former relates to the natural thinning process that many women experience as they grow older, whereby the hair gets noticeably thinner around the crown and forehead areas. This is a common occurrence in women once the onset of menopause starts and there is a marked increase in the percentage of women who suffer from this type of hair loss once they reach the age of 40. Once a woman reaches menopause, there is a marked decrease in levels of oestrogen and the effects of testosterone and DHT become more evident, which in turn leads to the thinning of hair around the crown and forehead areas. The life cycle of the hair follicles in these areas becomes shorter, and shedding of hair becomes more frequent. Hair shaft diameter as well as overall hair density decreases in women after menopause.

Figure 1 Hair microPigmentation Treatment (HPT) for male pattern baldness. (A) Before HPT and (B) after HPT
In addition to androgenetic alopecia, telogen effluvium is a common form of hair loss, which occurs when there is a change in the number of hair follicles growing hair. This condition appears as a diffuse thinning of hair on the scalp and can be more severe in some areas than others. Normally the hair on top of the scalp thins more than it does at the back and sides and there is usually no hairline recession. While hair can be noticeably thin in severe cases, people with telogen effluvium never completely lose all their scalp hair and the condition is fully reversible. The trigger factors for this form of hair loss are many and varied. It can happen to women soon after giving birth, when the sudden change in hormone levels is such a shock to the hair follicles that they shut down for a while. Additionally, physical trauma or having surgery can sometimes trigger this form of hair loss but arguably the two most common causes of this condition are chronic stress and diet deficiency.
Anagen effluvium, like telogen effluvium, is also a form of diffuse hair loss but develops much more rapidly and can cause individuals to lose all their hair. The condition is most frequently seen in people taking cytostatic drugs for cancer as they inhibit rapid cell proliferation resulting in a sudden shut down of hair fibre production. While the development of anagen effluvium is rapid, recovery from this type of hair loss can be equally as quick, because the follicles are frozen in time they will start to grow once the factor causing the anagen effluvium, such as medication, is removed.
A cause of hair loss that is more prevalent among women is traction alopecia. This is a gradual form of hair loss caused primarily by a pulling force being applied to the hair which commonly results from the individual frequently wearing their hair in particularly tight styles such as ponytails, pigtails, braids or the regular use of hair extensions. Additionally, wearing hairpieces that clip on in the same location can also cause this form of hair loss.
The causes of hair loss are varied, but the impact that the condition can have on an individuals self image and emotional well-being can be devastating. The harsh reality is that the psychological damage caused by hair loss can cause emotional stress that directly affects an individual’s physical health. Research carried out by Charité — Universitätsmedizin Berlin, one of the Europe’s largest teaching hospitals in Europe, found that hair loss could even lead to exaggerated feelings of ugliness and in extreme cases, lead to body dysmorphic disorder1. It is therefore unsurprising, that 60% of hair loss sufferers said they would rather have more hair than money or friends2.
Solutions for hair loss
Hair restoration surgery
According to the ISHRS 2013 Practice Census, it is estimated that 310000 surgical hair restoration procedures were performed worldwide in 2012, worth $1.9 billion3.
Follicular unit transplantation
Follicular unit transplantation (FUT) accounts for around two-thirds of all procedures. The FUT method involves the removal of a strip of skin with high density, permanent hair from the back of a patient’s scalp under local anaesthetic. Once the strip of skin has been removed from the donor area under a microscope, follicular units are separated which may contain one, two, three or four hairs — with the average yield being 2.2 hairs. Single hair grafts are used to create a natural hairline while the larger units are positioned in other areas to produce greater density. The area where the strip was removed is then closed using trichophytic closure, an advanced surgical technique in hair transplantation which allows hair to eventually grow through a linear donor scar, so the scar that remains is barely visible even in the case of shorter hairstyles. However, not everyone uses trichophytic closure and the scar will only remain barely visible when the procedure is carried out correctly. Additionally, when a trichophytic closure is used, it does not insure a narrow scar nor will it preclude a wide scar.
Once the grafts are prepared a surgeon will create tiny openings, between 0.7–0.9 mm (one hair graft) and 1.1–1.3 mm (three to four hair grafts)4, using a small gauge needle or specialised scalpel blade on the surface of the skin in the area of the scalp to be treated. Chisel point blades are preferable to spear point blades since they maintain incision width into the subcutaneous tissue and prevent compression of the bulbs. The follicular units are immediately transplanted to the prepared recipient sites one by one. It is important here that the follicular units are transplanted in a natural direction and that the transitions from existing areas of hair are as natural as possible. The transplanted follicular units establish themselves within a matter of days.
An FUT hair transplant can take between 4–12 hours depending on the number of grafts or hairs being transferred. Early results from the treatment can be seen after 3–4 months with final results commonly seen after 12–15 months.
Follicular unit extraction
The follicular unit extraction method (FUE) is a more recent method of transplantation surgery which involves the harvesting of individual hair grafts one at a time. This can be from almost every part of the body, although most typically from the back and sides of the scalp. The follicular units, comprising of one to four hairs, are removed from the donor area under local anaesthetic with a hollow punch. The punches that are used to harvest the grafts are 0.7–1.0 mm thin in diameter and owing to the use of these very small punches the area heals very quickly. In addition, the grafts are transplanted without changing the structure of the transplanted hair and result in a very natural look that is undetectable to the naked eye. The follicular units are then transplanted from the donor area to the target area one by one, similarly to the FUT method, and these units establish themselves within a couple of days.
The significant advantage to FUE is that there is no linear scar as seen with FUT. Unike the FUT method, the FUE method does not require a strip of skin to be removed, only very small dots are left in places where the follicular units were removed, which are hardly visible when the hair is shaved or cut to a few millimetres in length. FUE is a good method and is more appropriate where a smaller number of hairs are required. Where the strip method is not possible or where the patient wishes to maintain a very short hairstyle such as a number one or two shaved look. FUE is also good for repair or if a patient is ‘stripped out’ and unable to have further strips removed owing to scarring from prior FUT procedures.
However, FUE is a smaller procedure yielding less hair for a patient. Additionally, it is a lot more time consuming and is reliant on spreading the extractions over a large area of the scalp which significantly limits the number of grafts possible to transplant in a session compared to FUT. It can also require a surgeon to harvest donor grafts beyond the safe donor area, meaning that grafted hair follicles may grow but possibly not permanently. Resulting not only in losing the transplanted hairs, but also leaving visible FUE scars. An FUE transplant takes approximately 8 hours and during this time a maximum of around 1400–2000 follicular units can be transplanted. Should more transplanted units be required, it is usually possible to do this on consecutive treatment days.
In the UK, the combination of high-profile male celebrities who have undergone hair transplantation surgery coupled with the cost of treatment becoming more accessible to a growing number of hair loss sufferers has undoubtedly helped make more men in the UK open to the possibility of surgery and increase the number of procedures undertaken. Additionally, this has also encouraged more women to consider the option of investing in a transplant, with one London clinic claiming to have witnessed an 82% increase in the number of women undergoing hair transplants in the first 8 months of 2013, compared with the same period in 20115.
Since hair transplantation may be a good option for nearly 90%6 of male hair loss sufferers, many women think they are good candidates for hair transplant surgery, but this is usually not the case. According to the American Hair Loss Association, approximately only 2–5% of women will benefit from this type of procedure, owing to the fact that most women have diffuse hair loss6. This means that women have an overall thinning in all areas of the scalp, including the sides and back which are the areas that act as stable donor sites for men. However, in female pattern baldness these donor areas are usually unstable. This means that if the hair and accompanying follicles are removed from these donor areas in women and transplanted to another area on the scalp they are just going to fall out. The estimate of 2–5% may appear to be on the low side and according to the ISHRS Practice Census Results 2013, women made up 13.7% of hair restoration surgical patients3.
Medications
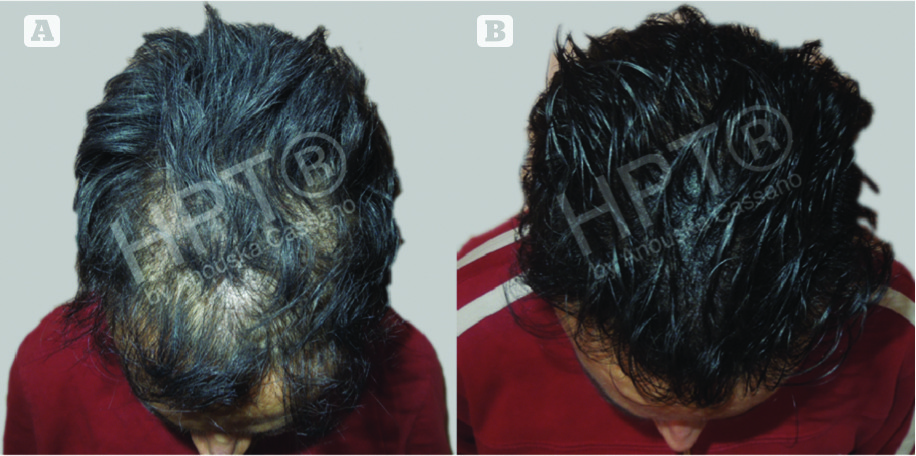
Figure 2 Hair microPigmentation Treatment (HPT) with hair restoration surgery. (A) Before HPT and (B) after HPT
There are some genuine solutions and medications available to help stop hair loss and even, in some cases, reverse the process partially. Successful treatment of hair loss using medications is greatly dependent on early intervention and it is important for the patient to begin treatment with an effective product as soon as they notice the onset of hair loss. Among all the options for non-surgical treatments for androgenetic alopecia only two, finasteride and minoxidil, have been approved by the US Food and Drug Administration (FDA).
The success of finasteride can be attributed to its ability to inhibit the enzyme that converts testosterone into DHT. Finasteride’s effects in slowing hair loss and stimulating new hair growth work best for early to moderate degrees of hair loss, but men with extensive hair loss are unlikely to experience much regrowth with use of this medication. Finasteride can reverse the miniaturisation process as well as prevent subsequent miniaturisation. Existing hair can also become thicker producing a much better coverage or density. It is important that the patient continues using finasteride or any positive effects will be gone within 6–12 months. This medication is generally well tolerated at low doses, but there have been reports when using a higher dosage of decreased libido, impotence, breast enlargement, stomach pain, gastrointestinal disorders, headaches, and rashes.
Finasteride is not approved for female use and in particular by women who are pregnant or who become pregnant as the drug has potential for interfering with the sexual development of a foetus.
Minoxidil works quite differently from finasteride as it is applied directly to the scalp, ideally twice daily. The lotion or foam dilates the blood vessels to the hair shafts to ensure that hairs can grow better. The results of minoxidil are negligible as it does not address the cause of the hair loss and only slightly delays the actual hair loss process, although the results tend to be more effective in women than in men.
Hair concealers
Hair loss concealers, which are widely available in most markets, are designed to cover up thinning areas of hair and can help disguise any apparent hair loss to give a full and voluminous look from a distance. Using a quality hair loss concealer can instantly give the illusion of thicker hair, giving the user greater confidence and can safely be used alongside any existing hair loss treatment or used to disguise transplant scarring.
However, there are obvious disadvantages to using concealers owing to the fact that they need to be applied daily, which is time consuming and will be washed out after a shower. Users of concealers repeat the application day after day which can ultimately become costly, but also acts as a reminder of their hair loss condition. Regular users of concealers often describe feelings of anxiety caused by the fear of being ‘found out’ with makeup running in the rain, sweating during physical activities or stains left on shirt collars and pillow cases. Although most modern versions of concealers are far more durable than previous versions there is still the risk that it can start coming off when the user least expects. Since concealers obviously don’t give the illusion of hair follicles, they are only undetectable from a distance and cannot work with very short hair or crop cuts.
Hair systems
Hair systems, hair replacement systems, hairpieces, toupees and wigs are often used interchangeably and all refer to the same non-surgical hair restoration procedure where human or synthetic hair is added to a thin base or foundation, which in turn is attached to the scalp by varying methods. The latest hair systems can look very natural and virtually undetectable. They can work very well for almost anyone with hair loss, and if done properly, the wearer can have a natural looking head of hair in relatively little time that can be styled in the way they prefer. It is no longer true that hair systems make people look like they are wearing a ‘rug’ on their head.
Hair systems are often custom made, as each wearer will have different needs and varying lifestyles, and are manufactured using human, remy, synthetic, cyber or robo hair. The cost of a top-end custom made system can, however, run into thousands of pounds. Systems are attached to the scalp or balding area most commonly using double sided tapes and liquid adhesives, sometimes referred to as bonding. Weaving was previously used as a method, where the hair system is literally weaved into the patients existing hair, but in recent years many believe weaving causes traction alopecia resulting in very few companies using this method of attachment.
One of the biggest drawbacks with hair systems is that the cost of maintaining them is typically high and can be very time consuming. Maintenance issues can range from periodic cleaning, adding hair, re-colouring, to daily attachment hassles with tapes, glues, adhesives, and clips. Most people think that a hair system is a one‑off investment. This is not the reality and a hair system can ultimately be a very costly option for hair loss sufferers. Hair systems that look and feel the most natural are also the most expensive and the least durable and may last only 12 months. Maintenance can be quite costly too, sometimes over a hundred pounds a month when it comes to changing a system front, adding hair or re-colouring.
Hair microPigmentation Treatment

Figure 3 Hair microPigmentation Treatment (HPT) for transplant scarring. (A) Before HPT and (B) after HPT
Hair microPigmentation Treatment (HPT®), more commonly known as scalp micropigmentation or scalp tattooing, is a revolutionary semi-permanent micro-pigmenting technique that offers an alternative option for both men and women suffering from hair loss who are not appropriate candidates for hair transplant surgery or who do not want it. HPT involves the use of a digitally controlled needle that applies medical grade hypoallergenic colour pigment into the scalp.
Unlike a traditional tattoo that would use ‘ink’, HPT is performed using specially designed pigments that will not have the colour change or migration (blurring) that is commonly seen with a body art tattoo. Although it may appear to be a similar technique, the needles and treatment depth into the skin are very different. Both use needles to implant colour, but that is where the similarity ends. Traditional body art tattoos do have the tendency to change colour. If it was black to start with, very often they will turn blue as a result of migration owing to the type of ink used and the tissue level the tattoo was implanted. HPT is not implanted at a deep level on the scalp and the simulated hair follicles are implanted in the very top layers of the epidermis.
HPT is designed to last a number of years and typically we would expect this treatment to last between 1–3 years with some minor maintenance or touch ups. However, it is impossible to predict the exact length of time the treatment will last, as each patient is different and lifestyle choice and other variables can effect the treatment in individual cases. The pigments used are designed to fade over time, this makes it possible to adjust the tone and change the hairline to be more ‘age appropriate’ for patients as they mature.
HPT is a multi-treatment procedure which will usually require 2–3 sessions to complete the overall treatment for the best results. Depending on the size of the area to be treated and the extent of a patient’s hair loss, each session will take 2–4 hours. The treatment in itself is not painful as the pigment is only implanted in the dermis and not a deeper depth like a body art tattoo, but it is advisable to not work longer than in 4 hour sessions as it is a residual build up of ‘irritation’ that can eventually make the scalp feel sore.
Scalp micropigmentation to date has most widely been used as a hair loss solution for male pattern baldness. In the majority of cases the procedure is used to give the patient the illusion of a closely shaven head or cropped appearance. However, as a complimentary hair loss solution, HPT can be effectively used to camouflage transplant scarring from surgery, enhance hair restoration procedures or camouflage diffuse thinning and hair loss specifically for women.
HPT for male pattern baldness
HPT can create the illusion of either denser looking hair, creating a hairline or even full head coverage ‘shaven look’ that may have been previously unachievable for the patient with other hair loss solutions. The hairline is the most important part of the scalp micropigmentation treatment, as this is the focal point, and will determine the overall look. If not done correctly the treatment will look unnatural and fake. It is important to take a consultative approach with the patient to work with them to design, mark, measure, and approve each hairline before any pigment is implanted. Some patients may wish for a very defined hairline, but we often advise them to try a more natural look that takes into account age-appropriateness and ethnicity.
HPT with transplant surgery
HPT can be used to enhance any successful hair restoration surgery, either FUE or FUT, by creating the illusion of thicker ‘hair’ at root level and infilling between transplanted grafts. A growing number of our HPT procedures are referrals from surgeons where the patient did not have enough donor hair for surgery or required the illusion of additional density to improve the overall result of their transplant.
HPT for transplant scarring
We have used HPT to effectively treat a number of patients to camouflage scarring, including either strip scarring, hole punch or plug marks left after hair transplant surgery. The pigment is implanted into the scar tissue, matching the hair follicles and hair surrounding it, and depending on the type of scar that needs camouflaging the pigment will be blended into the hair surrounding the scar for a more natural look. Scar tissue is very different in composition to that of healthy skin and can be unpredictable in how it reacts to scalp micropigmentation treatment and retention of the implanted pigment. HPT is only appropriate for the treatment of scars more than a year old that are fully healed.
HPT for female diffuse thinning

Figure 4 Hair microPigmentation Treatment for female hair loss. (A) Before HPT and (B) after HPT
As highlighted previously, female hair loss sufferers are particularly limited in the solutions available to them. This condition can be devastating for women in particular, who often feel self-conscious and isolated when experiencing hair loss. Female hair loss is a problem that is affecting an ever-increasing number of women associated with modern lifestyles and varying underlying medical conditions. HPT has immediate results and will create the illusion of thicker hair, taking the focus away from the scalp or bare patches and reduces the time and pressure on the patient of having to hide these thinning or bare patches under headwear or ensuring their hairstyle is always ‘exact’ to cover these areas. Additionally, the illusion of ‘hair’ follicles from HPT far surpasses the results achievable from any concealer product on close inspection, with no need for daily application. It also eliminates the fear factor of being ‘found out’, giving the patient the freedom to engage with physical and social activities with confidence.
Conclusions
Awareness of HPT or scalp micropigmentation as a potential solution for hair loss sufferers, in particular, women suffering from diffuse thinning, is currently low. Indeed, a number of industry bodies and hair loss charities do not acknowledge this treatment alongside other alternative solutions on their websites.
The author firmly believes that all scalp micropigmentation practitioners should have a comprehensive understanding and knowledge of hair loss causes and the broad range of hair loss solutions, both surgical and non-surgical, which are available to patients. Only by having an in-depth knowledge of hair loss causes and the broader treatments available can practitioners give a holistic recommendation for the best solution or course of treatment that is right for the patient. In a number of cases this will be HPT, as the majority of patients the author sees and treats have already explored other hair loss solutions. However, for a few patients the best course of treatment will be HPT in combination with another solution such as hair restoration surgery, or not HPT at all.
The quality of consultation for this treatment is of vital importance. To this end, the author’s approach is endorsed by Glenn M. Callaghan, PhD Professor of Psychology and Director of Clinical Training at the Department of Psychology at San Jose State University. The more time you invest with your patient, really listening to and understanding their hair loss situation and history at the consultation stage, the more likely they are to be satisfied with the final result. If a patient has emotional or psychological issues, the likely outcome is that they will not be satisfied or happy with any scalp micropigmentation treatment you perform. To understand if a potential patient has body image disorders the author recommends the use of the Body Image Psychological Inflexibility Scale (BIPIS)7 to ascertain a patient’s suitability for treatment.
The author always stresses that although the treatment can create the illusion of hair or hair density, it is not actual hair. If a patient is a suitable candidate for hair restoration surgery and can afford it, practitioners should recommend this as the route they should take. Hair loss sufferers, if they could turn back the clock, would always choose the time in their life when they had a full head of natural hair.
One of the key strengths of HPT is its potential usage in combination with other hair loss solutions to help patients realise their hair loss goals. Whether this is women using the treatment in combination with continued use of hair concealers or patients who have undergone hair restoration surgery looking to create the illusion of additional density to enhance the overall result of their transplant.
It is in the area of working with hair restoration clinics that the greatest synergy when promoting the benefits of HPT as a combination treatment can be witnessed. One of the most common complaints that patients have after hair transplant surgery is that the density of their transplant was less than they expected, with 64.1% highlighting this factor3. An increasing number of hair transplantation clinics are starting to see the value of offering scalp micropigmentation as an additional service to their patients, either as a complimentary treatment to create the illusion of additional density, enhance the overall result of the surgical procedure or increase patient satisfaction, as well as a standalone solution for both male and female hair loss patients who were unsuitable candidates for hair restoration surgery that they previously may have been unable to treat at the clinic.
Currently, scalp micropigmentation is unregulated and there is little in the way of quality control or standards. To address this the author has developed HPT scalp micropigmentation into a training course, which is the only course of its kind to have been independently endorsed by the pertinent industry bodies. The course has been specifically designed for hair restoration clinics and their surgical teams. By improving the quality of scalp micropigmentation, raising standards and making the treatment more accessible to patients through hair restoration clinics the author hopes that the industry bodies, such as the ISHRS, and hair loss charities will start to acknowledge and promote scalp micropigmentation alongside other more established hair loss solutions as an option for individuals suffering from hair loss.

